Isolated Spinal Cord Neurosarcoidosis Diagnosed by Cord Biopsy and Thalidomide Trial
- Affiliations
-
- 1Department of Neurology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 2Department of Neurosurgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. ybkim1218@cau.ac.kr
- KMID: 1777993
- DOI: http://doi.org/10.3346/jkms.2011.26.1.154
Abstract
- We report a case of 54-yr-old woman who presented with 4-extremities weakness and sensory changes, followed by cervical spinal cord lesion in magnetic resonance imaging. Based on the suspicion of spinal tumor, spinal cord biopsy was performed, and the histology revealed multinucleated giant cells, lymphocytes and aggregated histiocytes within granulomatous inflammation, consistent with non-caseating granuloma seen in sarcoidosis. The patient was treated with corticosteroid, immunosuppressant and thalidomide for years. Our case indicates that diagnosis of spinal cord sarcoidosis is challenging and may require histological examination, and high-dose corticosteroid and immunosuppressant will be a good choice in the treatment of spinal cord sarcoidosis, and the thalidomide has to be debated in the spinal cord sarcoidosis.
MeSH Terms
-
Adrenal Cortex Hormones/therapeutic use
Biopsy
Central Nervous System Diseases/drug therapy/pathology
Female
Humans
Immunosuppressive Agents/*therapeutic use
Magnetic Resonance Imaging
Middle Aged
Sarcoidosis/drug therapy/pathology
Spinal Cord/*pathology
Spinal Cord Diseases/drug therapy/*pathology
Thalidomide/*therapeutic use
Figure
-
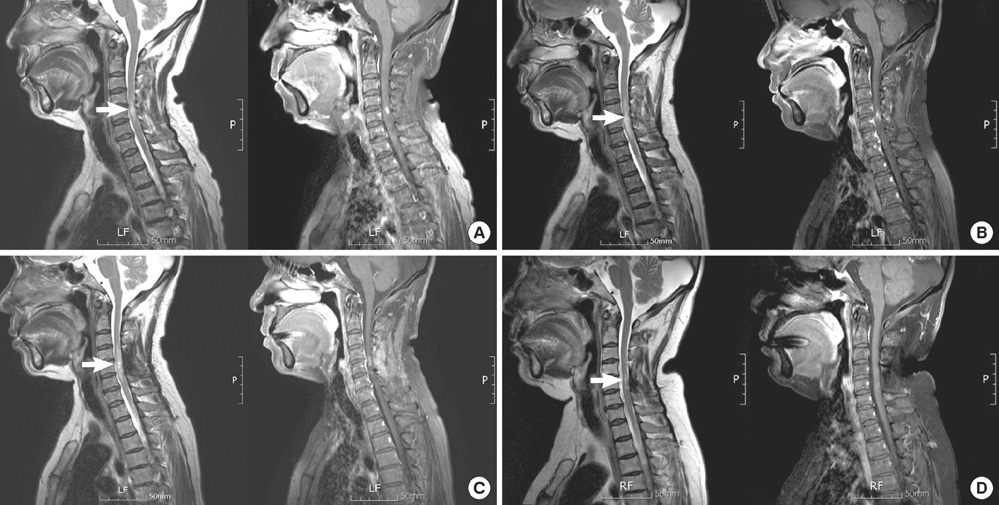
Fig. 1 T2-weighted and gadolinium enhanced T1-weighted cervical MRI in the patient. (A) Initial cervical spine MRI (magnetic resonance image) revealed increased T2 signal from C4 to C6 level, edematous expansion of the cord and intense nodular enhancement. Based on the MRI, spinal cord tumor, demyelinating disease and acute tranverse myelitis were suspected. (B) One month later, the follow-up spinal MRI showed the extended lesion relative to previous MRI, and which highly suggested the spinal cord tumor such as intramedullay astrocytoma. (C) Demonstrates cervical spine MRI after laminectomy and tissue biopsy. (D) The patient was treated with high-dose corticosteroid and immunosuppressant for over 2 yr and spinal cord lesion was much resolved in MRI.

Fig. 2 Histopathology of the biopsied cervical cord lesion. (A) The specimen biopsied from the lesion contained multinucleated giant cells (red arrows), lymphocytes (black arrow) and aggregated histiocytes (white arrow) within granulomatous inflammation, consistent with non-caseating granuloma seen in sarcoidosis (H&E staining × 200). (B) The AFB staining of the specimen did not show the mycobacterium tuberculosis. PAS staining did not reveal the fungus.
Reference
-
1. Baughman RP, Lower EE, du Bois RM. Sarcoidosis. Lancet. 2003. 361:1111–1118.2. Stern BJ. Neurological complications of sarcoidosis. Curr Opin Neurol. 2004. 17:311–316.3. Hoitsma E, Faber CG, Drent M, Sharma OP. Neurosarcoidosis: a clinical dilemma. Lancet Neurol. 2004. 3:397–407.4. Joseph FG, Scolding NJ. Neurosarcoidosis: a study of 30 new cases. J Neurol Neurosurg Psychiatry. 2009. 80:297–304.5. Shah R, Roberson GH, Curé JK. Correlation of MR imaging findings and clinical manifestations in neurosarcoidosis. AJNR Am J Neuroradiol. 2009. 30:953–961.6. Varron L, Broussolle C, Candessanche JP, Marignier R, Rousset H, Ninet J, Sève P. Spinal cord sarcoidosis: report of seven cases. Eur J Neurol. 2009. 16:289–296.7. Scott TF, Yandora K, Valeri A, Chieffe C, Schramke C. Aggressive therapy for neurosarcoidosis: long-term follow-up of 48 treated patients. Arch Neurol. 2007. 64:691–696.8. Caneparo D, Lucetti C, Nuti A, Cipriani G, Tessa C, Fazzi P, Bonuccelli U. A case of sarcoidosis presenting as a non-specific intramedullary lesion. Eur J Neurol. 2007. 14:346–349.9. Bhagavati S, Choi J. Intramedullary cervical spinal cord sarcoidosis. Spinal Cord. 2009. 47:179–181.10. Maroun FB, O'Dea FJ, Mathieson G, Fox G, Murray G, Jacob JC, Reddy R, Avery R. Sarcoidosis presenting as an intramedullary spinal cord lesion. Can J Neurol Sci. 2001. 28:163–166.11. Hammond ER, Kaplin AI, Kerr DA. Thalidomide for acute treatment of neurosarcoidosis. Spinal Cord. 2007. 45:802–803.12. Viñas FC, Rengachary S, Kupsky WJ. Spinal cord sarcoidosis: a diagnostic dilemma. Neurol Res. 2001. 23:347–352.13. Zajicek JP, Scolding NJ, Foster O, Rovaris M, Evanson J, Moseley IF, Scadding JW, Thompson EJ, Chamoun V, Miller DH, McDonald WI, Mitchell D. Central nervous system sarcoidosis-diagnosis and management. QJM. 1999. 92:103–117.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spinal Cord Neurosarcoidosis after Cervical Compressive Myelopathy
- Spontaneous Herniation of the Thoracic Spinal Cord: A Case Report
- Intramedullary Spinal Cord Cavernous Hemangiomas Presented With Radiculopathy
- Cervical spinal cord injury by the impingement of fractured lamina
- Spinal cord compression with paraparesis in ovarian cancer patient
