Clinical Implication of Surgical Resection for the Rare Cardiac Tumors Involving Heart and Great Vessels
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. kkh726@snu.ac.kr
- KMID: 1777559
- DOI: http://doi.org/10.3346/jkms.2013.28.5.717
Abstract
- This study aimed to investigate the clinical implication of surgical resection for the malignancies of heart and great vessels. Between January 2001 and May 2011, a retrospective review of the results in 12 patients was conducted. There were 6 patients with primary cardiac tumor including leiomyosarcoma, angiosarcoma, undifferentiated type sarcoma and malignant fibrous histiocytoma. The remaining 6 patients had the metastatic tumors or adjacent invasion to the heart and great vessels. Six of seven patients who underwent complete resection had no evidence of recurrence. However, four of five patients who underwent incomplete resection or biopsy showed local recurrence or distant metastasis of residual tumor, and one of them required reoperation for recurred tumor. In-hospital mortality was 8.3% and the mean survival of all patients was 22.2 +/- 6.1 months. Survival of the incomplete resection group, except for the two biopsy cases, was 25.9 +/- 7.9 months, and there was no mortality in the complete resection group. Therefore, clinical outcomes in patients who had malignancies of the heart and great vessels may be improved when the aggressive and complete resection, or possible debulking for palliation, was performed. Moreover, adjuvant multimodality therapy may be imperative to prevent recurrence or metastasis, and to provide improved survival.
MeSH Terms
-
Adult
Aged
Female
Follow-Up Studies
Heart Neoplasms/mortality/pathology/*surgery
Humans
Intensive Care Units
Kaplan-Meier Estimate
Length of Stay
Magnetic Resonance Imaging
Male
Middle Aged
Neoplasm Recurrence, Local
Neoplasm Staging
Retrospective Studies
Sarcoma/mortality/pathology/*surgery
Tomography, X-Ray Computed
Figure
-
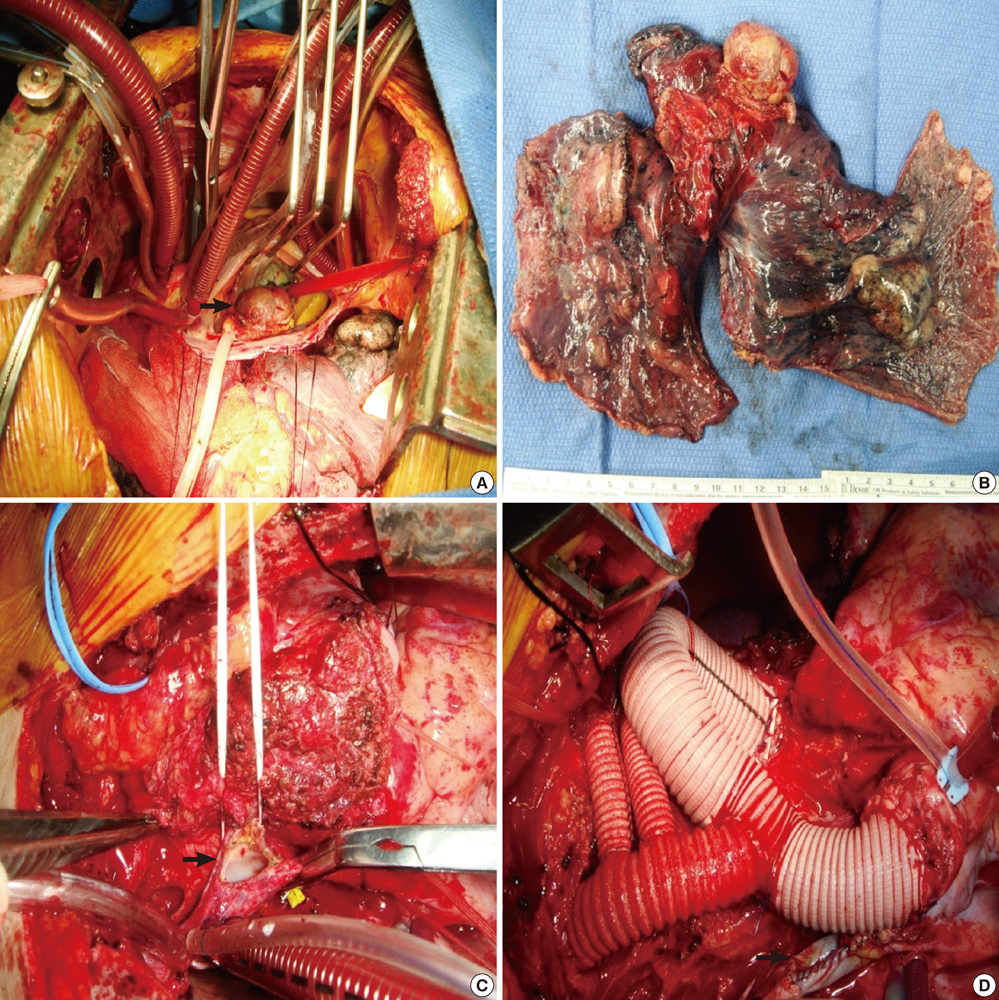
Fig. 1 Intraoperative findings and surgical resection. (A) This picture shows the metastatic tumor originated from colon cancer which involved the LA and right lung. The tumor causes the obstruction of mitral valve (arrow). (B) En bloc tumor resection with intra-pericardial bilobectomy of right middle and lower lobe, LA plasty with glutaraldehyde (GA)-fixed autologous pericardial patch, mediastinal lymph node dissection. (C) Mediastinal mass involves the distal ascending aorta, total arch and arch vessels, superior vena cava, and innominate vein. Resection of superior vena cava (SVC) invasion (arrow). (D) Replacement of the ascending aorta and total arch with 18 mm vascular graft, and separate replacement of arch vessels using 12-8-8 mm Y-Yed graft (Spielvogel technique). SVC reconstruction with GA-fixed autologous pericardium (arrow).

Fig. 2 Kaplan-Meier survival curves for the overall survival rate for all patients with malignant tumor of the heart and great vessels.

Fig. 3 Preoperative cardiac MRI and intraoperative findings of malignant cardiac tumor. (A) Well enhancing 4.8-cm size broad based mass in left atrium (LA) and interatrial septum extending to orifice of left lower pulmonary vein. (B) Tumor involvement to mitral valve anterior leaflet (arrow). (C) SVC transection with RA retraction, and LA roof approach for full exposure of mass: Broad based, 5×3 cm sized, multilobulating, large LA mass occupied the LA cavity including posterior and inferior wall, and invaded the mitral valve leaflet.
Reference
-
1. Neragi-Miandoab S, Kim J, Vlahakes GJ. Malignant tumours of the heart: a review of tumour type, diagnosis and therapy. Clin Oncol (R Coll Radiol). 2007. 19:748–756.2. Silverman NA. Primary cardiac tumor. Ann Surg. 1980. 191:127–138.3. Dohi T, Ohmura H, Daida H, Amano A. Primary right atrial cardiac osteosarcoma with congestive heart failure. Eur J Cardiothorac Surg. 2009. 35:544–546.4. Nayar S, Nayar PG, Cherian K. Angiosarcoma presenting as syncope. Asian Cardiovasc Thorac Ann. 2008. 16:154–156.5. Yoshitake I, Hata M, Sezai A, Niino T, Unosawa S, Shimura K, Kasamaki Y, Minami K. Cardiac angiosarcoma with cardiac tamponade diagnosed as a ruptured aneurysm of the sinus valsalva. Jpn J Clin Oncol. 2009. 39:612–615.6. Kitamura A, Ozaki N, Mukohara N, Yoshida M, Shida T. Primary cardiac liposarcoma causing cardiac tamponade: report of a case. Surg Today. 2007. 37:974–976.7. Park BJ, Bacchetta M, Bains MS, Downey RJ, Flores R, Rusch VW, Girardi LN. Surgical management of thoracic malignancies invading the heart or great vessels. Ann Thorac Surg. 2004. 78:1024–1030.8. Talbot SM, Taub RN, Keohan ML, Edwards N, Galantowicz ME, Schulman LL. Combined heart and lung transplantation for unresectable primary cardiac sarcoma. J Thorac Cardiovasc Surg. 2002. 124:1145–1148.9. Bakaeen FG, Jaroszewski DE, Rice DC, Walsh GL, Vaporciyan AA, Swisher SS, Benjamin R, Blackmon S, Reardon MJ. Outcomes after surgical resection of cardiac sarcoma in the multimodality treatment era. J Thorac Cardiovasc Surg. 2009. 137:1454–1460.10. Bear PA, Moodie DS. Malignant primary cardiac tumors: the Cleveland Clinic experience, 1956 to 1986. Chest. 1987. 92:860–862.11. Mayer F, Aebert H, Rudert M, Königsrainer A, Horger M, Kanz L, Bamberg M, Ziemer G, Hartmann JT. Primary malignant sarcomas of the heart and great vessels in adult patients--a single-center experience. Oncologist. 2007. 12:1134–1142.12. Zhang PJ, Brooks JS, Goldblum JR, Yoder B, Seethala R, Pawel B, Gorman JH, Gorman RC, Huang JH, Acker M, et al. Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival. Hum Pathol. 2008. 39:1385–1395.13. Spielvogel D, Strauch JT, Minanov OP, Lansman SL, Griepp RB. Aortic arch replacement using a trifurcated graft and selective cerebral antegrade perfusion. Ann Thorac Surg. 2002. 74:S1810–S1814.14. Blackmon SH, Rice DC, Correa AM, Mehran R, Putnam JB, Smythe WR, Walkes JC, Walsh GL, Moran C, Singh H, et al. Management of primary pulmonary artery sarcomas. Ann Thorac Surg. 2009. 87:977–984.15. Shanmugam G. Primary cardiac sarcoma. Eur J Cardiothorac Surg. 2006. 29:925–932.16. Kubota H, Takamoto S, Kotsuka Y, Miyairi T, Murakawa T, Makuuchi H, Kawauchi M, Furuse A, Sudo K. Surgical treatment of malignant tumors of the right heart. Jpn Heart J. 2002. 43:263–271.17. Butany J, Nair V, Naseemuddin A, Nair GM, Catton C, Yau T. Cardiac tumors: diagnosis and management. Lancet Oncol. 2005. 6:219–228.18. Debourdeau P, Gligorov J, Teixeira L, Aletti M, Zammit C. Malignant cardiac tumors. Bull Cancer. 2004. 91:136–146.19. Kim CH, Dancer JY, Coffey D, Zhai QJ, Reardon M, Ayala AG, Ro JY. Clinicopathologic study of 24 patients with primary cardiac sarcomas: a 10-year single institution experience. Hum Pathol. 2008. 39:933–938.20. Eckstein R, Gössner W, Rienmüller R. Primary malignant fibrous histiocytoma of the left atrium: surgical and chemotherapeutic management. Br Heart J. 1984. 52:354–357.21. Burke A, Virmani R. Tumors of the heart and great vessels. Atlas of tumor pathology. 3rd series. 1996. Washington, D.C.: Armed Forces Institute of Pathology.22. Kim MP, Correa AM, Blackmon S, Quiroga-Garza G, Weilbaecher D, Bruckner B, Ramlawi B, Rice DC, Vaporciyan AA, Reardon MJ. Outcomes after right-side heart sarcoma resection. Ann Thorac Surg. 2011. 91:770–776.23. Putnam JB Jr, Sweeney MS, Colon R, Lanza LA, Frazier OH, Cooley DA. Primary cardiac sarcomas. Ann Thorac Surg. 1991. 51:906–910.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Congenitally Corrected Transposition of Great Arteries: Morphologic and Functional Evaluation with Cardiac CT
- Congenitally Corrected Transposition of the Great Arteries
- Angiosarcoma in Right Atrium
- A Case of Corrected Transposition of Great Vessels, Associated with itral?Insufficiency
- A case of malignant fibrous histiocytoma with invasion into great vessels and heart which was confused with benign myxoma
