Imperforate Anus: Determination of Type Using Transperineal Ultrasonography
- Affiliations
-
- 1Department of Radiology, Seoul National University Children's Hospital, Seoul 110-744, Korea. kimio@snu.ac.kr
- KMID: 1777263
- DOI: http://doi.org/10.3348/kjr.2009.10.4.355
Abstract
OBJECTIVE
This study was designed to assess the usefulness of transperineal ultrasonography (US) for the determination of imperforate anus (IA) type.
MATERIALS AND METHODS
From January 2000 to December 2004, 46 of 193 patients with an IA underwent transperineal US prior to corrective surgery. Sonographic findings were reviewed to identify the presence of internal fistulas and to determine "distal rectal pouch to perineum (P-P)" distances. IA types were determined based on the sonographic findings, and the diagnostic accuracy of transperineal US was evaluated based on surgical findings.
RESULTS
Of the 46 patients, 17 patients were surgically confirmed as having a high-type IA, three patients were confirmed as having an intermediate-type IA and 26 patients were confirmed as having a low-type IA. The IA type was correctly diagnosed by the use of transperineal US in 39 of the 46 patients (85%). In 14 of the 17 patients with a high-type IA, internal fistulas were correctly identified. All cases with a P-P distance > 16 mm were high-type IAs and all cases with a P-P distance < 5 mm were low-type IAs.
CONCLUSION
Transperineal US is a good diagnostic modality for the identification of internal fistulas in cases of high-type IA and for defining the IA level.
Keyword
MeSH Terms
Figure
-

Fig. 1 Transperineal sonography of normal female anatomy is shown. Transperineal sonogram from normal one-week-old girl showing bladder (B), symphysis pubis (S) and vagina (V) between urethra (U) and rectum (R) and normal rectum directing posteriorly to anus is shown. Echogenic fat plane was present between rectum and vagina (arrow).

Fig. 2 Schematic diagram of various internal fistulas for male and female imperforate anus is presented.
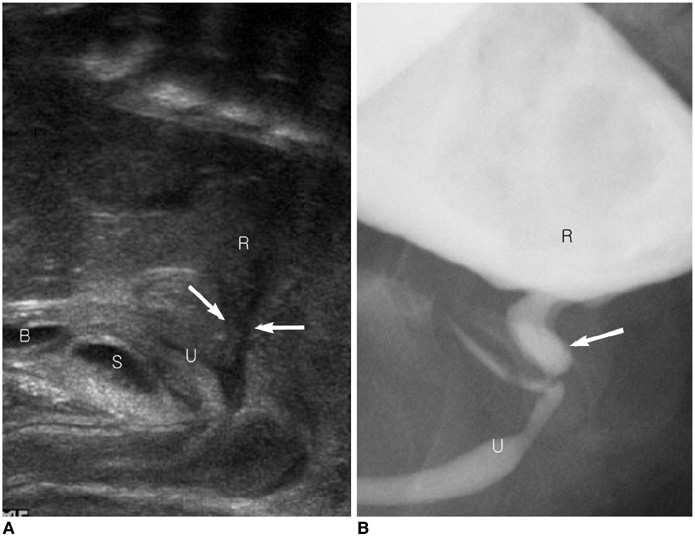
Fig. 3 Findings for high-type imperforate anus with recto-urethral fistula are shown. A. Transperineal sonogram shows low echogenic fistula (arrows) between rectum and urethra. B. Distal colostogram shows rectoposterior urethral fistula (arrow), which was correlated with US findings.
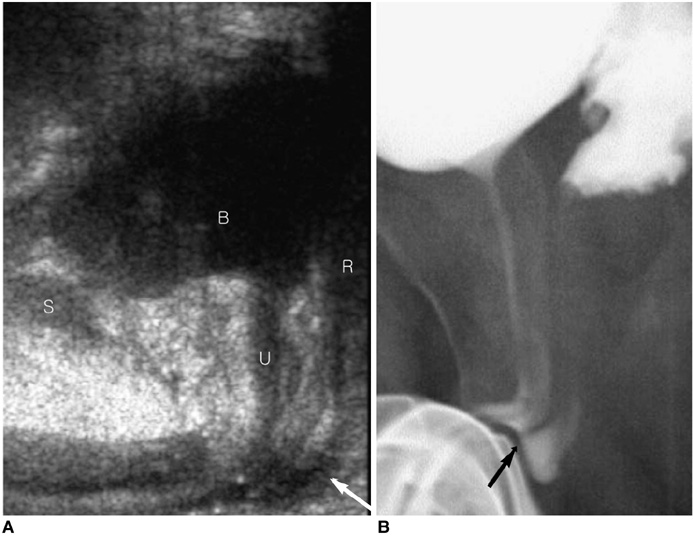
Fig. 4 Findings for intermediate-type imperforate anus with recto-bulbar urethral fistula are shown. A. Transperineal US shows long low echoic fistula tract (arrow) between rectum and bulbous urethra. B. Retrograde urethrogram shows fistula (arrow) between rectum and bulbous urethra.

Fig. 5 Findings for low-type imperforate anus with anocutaneous fistula are shown. Distal rectum (arrows) abnormally courses towards perineum, anterior to normal location of anus.
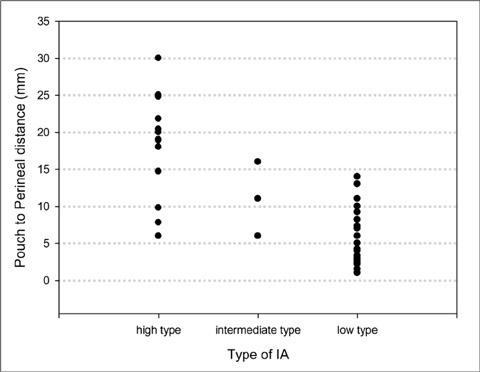
Fig. 6 Pouch to perineum distance according to imperforate anus type is plotted. Some overlap of pouch to perineum distances was observed among imperforate anus types. However, all cases with pouch to perineum distance > 16 mm were high-type imperforate anus and all cases with pouch to perineum distance < 5 mm were low-type imperforate anus.
Reference
-
1. Donaldson JS, Black CT, Reynolds M, Sherman JO, Shkolnik A. Ultrasound of the distal pouch in infants with imperforate anus. J Pediatr Surg. 1989. 24:465–468.2. Teele RL, Share JC. Transperineal sonography in children. AJR Am J Roentgenol. 1997. 168:1263–1267.3. Kim IO, Han TI, Kim WS, Yeon KM. Transperineal ultrasonography in imperforate anus: identification of the internal fistula. J Ultrasound Med. 2000. 19:211–216.4. Oppenheimer DA, Carroll BA, Shochat SJ. Sonography of imperforate anus. Radiology. 1983. 148:127–128.5. Santulli TV, Kiesewetter WB, Bill AH Jr. Anorectal anomalies: a suggested international classification. J Pediatr Surg. 1970. 5:281–287.6. Stephens FD, Smith ED. Classification, identification, and assessment of surgical treatment of anorectal anomalies. Pediatr Surg Int. 1986. 1:200–205.7. Berdon WE, Baker DH, Santulli TV, Amoury R. The radiologic evaluation of imperforate anus. An approach correlated with current surgical concepts. Radiology. 1968. 90:466–471.8. Ikawa H, Yokoyama J, Sanbonmatsu T, Hagane K, Endo M, Katsumata K, et al. The use of computerized tomography to evaluate anorectal anomalies. J Pediatr Surg. 1985. 20:640–644.9. Mezzacappa PM, Price AP, Haller JO, Kassner EG, Hansbrough F. MR and CT demonstration of levator sling in congenital anorectal anomalies. J Comput Assist Tomogr. 1987. 11:273–275.10. McHugh K, Dudley NE, Tam P. Pre-operative MRI of anorectal anomalies in the newborn period. Pediatr Radiol. 1995. 25:S33–S36.11. Schuster SR, Teele RL. An analysis of ultrasound scanning as a guide in determination of "high" or "low" imperforate anus. J Pediatr Surg. 1979. 14:798–800.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound measurement of pouch to perineum distance as a guide in determination of high or low imperforate anus
- Two Experiences of Operation about Urogenital Anomalies Associated with Congenital Imperforate Anus
- A case of successful vaginal delivery in a patient with a repair of an imperforate anus
- Colonic Web Associatd with Imperforate Anus
- Urogenital anomalies associated with imperforative anus
