Two Cases of an Implantation of a Permanent Pacemaker Using a Transaxillary Incision
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Pusan National University Hospital, Busan, Korea. mdjunkim@yahoo.co.kr
- 2Department of Thoracic and Cardiovascular Surgery, Pusan National University School of Medicine, Pusan National University Hospital, Busan, Korea.
- KMID: 1776352
- DOI: http://doi.org/10.4070/kcj.2008.38.9.500
Abstract
- In surgeries that require the implantation of a pacemaker, the endocardial pacemaker leads are introduced into the cardiac chambers through subclavian or axillary venous catheterization or cephalic vein cutdown. The drawback of this type of surgery is scarring of the pectoral area, which can be a serious cosmetic problem especially for young women. In this study, we report on 2 cases where a permanent pacemaker in two young women with symptomatic bradycardia was implanted using a transaxillary incision. Both patients successfully recovered with no complications and were asymptomatic for more than 17 months after the procedure. Therefore, we found that implantation of a pacemaker via transaxillary incision provided excellent cosmetic results and should be considered in young women that require this type of surgery.
MeSH Terms
Figure
-
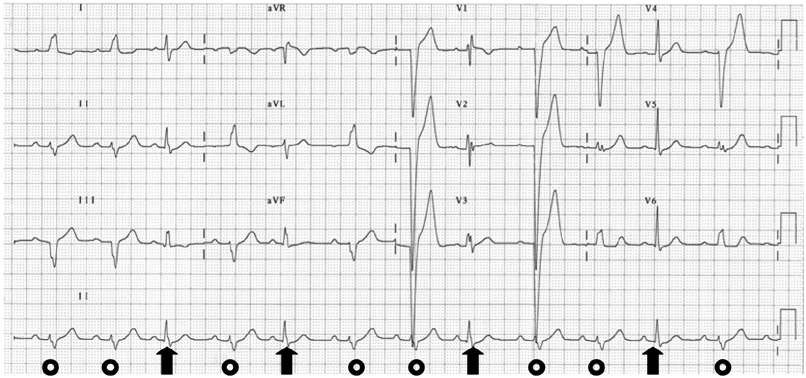
Fig. 1 Twelve-lead electrocardiogram showing a sinus rhythm and an alternating bundle branch block {Left bundle branch block (◯) and right bundle branch block (↑)}.
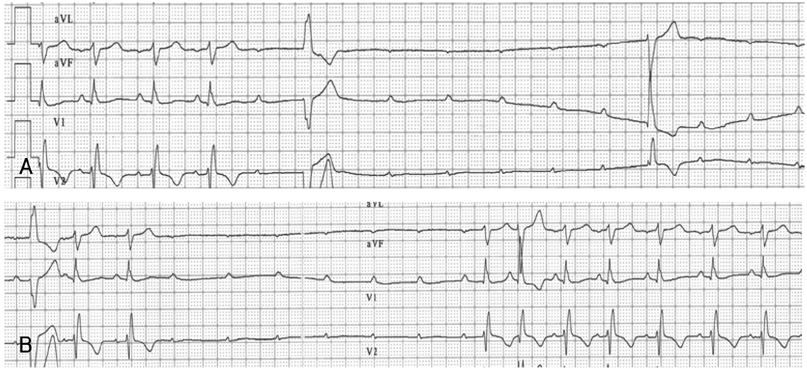
Fig. 2 Electrocardiographic findings of case 1. Electrocardiograms (aVF, V1 and V2 leads) showing a sinus rhythm with complete blockage of the right bundle branch, followed by type-II second-degree AV block and a long duration of ventricular asystole (A). A high-grade AV block that was spontaneously resolved (B).
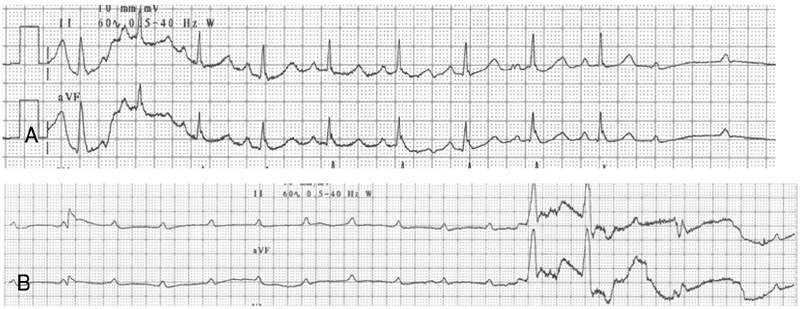
Fig. 3 Electrocardiographic findings of case 1 eleven days after presentation. Electrocardiogram showing a type-II second-degree AV blockage with a long ventricular aystole (A and B) accompanied by seizure-like motions of the patient.
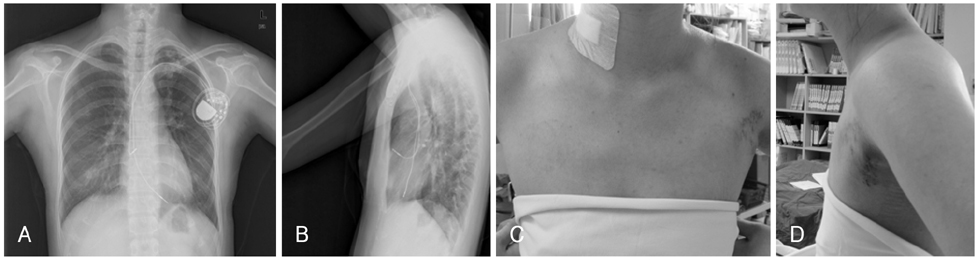
Fig. 4 Images of case 1 after pacemaker implanatation. The chest X-ray showed that the leads were appropriately implanted without any complications (A and B). The pacemaker pocket wound is along the anterior axillary line (C and D).
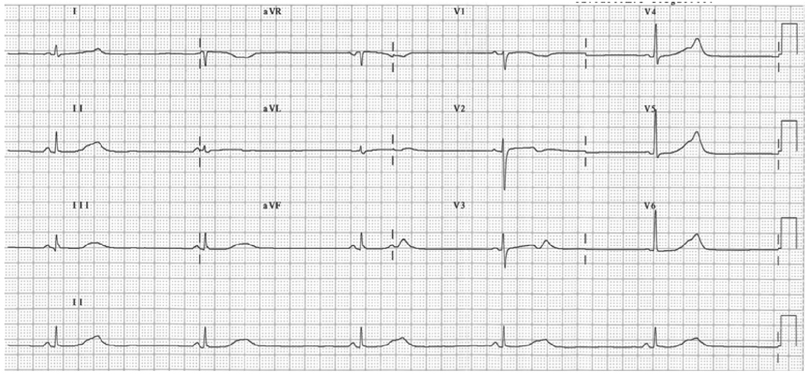
Fig. 5 Twelve-lead electrocardiogram of case 2 showing sinus bradycardia.

Fig. 6 Twenty-four hour Holter electrocardiogram showing a marked sinus bradycardia followed by a single premature ventricular beat (third QRS complex) and then a premature ventricular beat (fifth QRS complex) initiating polymorphic ventricular tachycardia (↔).

Fig. 7 Images of case 2 after pacemaker implanatation. The chest X-ray showed that the leads were appropriately implanted without complication (A and B). The pacemaker pocket is invisible from the anterior view (C) and located along the anterior axillary line (D).
Reference
-
1. Furman S. Venous cutdown for pacemaker implantation. Ann Thorac Surg. 1986. 41:438–439.2. Miler FA Jr, Holmes DR Jr, Gersh BJ, Maloney JD. Permanent transvenous pacemaker implantation via the subclavian vein. Mayo Clin Proc. 1980. 55:309–314.3. Ramza BM, Rosenthal L, Hui R, et al. Safety and effectiveness of placement of pacemaker and defibrillator leads in the axillary vein guided by contrast venography. Am J Cardiol. 1997. 80:892–896.4. Jones DG, Stiles MK, Stewart JT, Armstrong GP. Ultrasound-guided venous access for permanent pacemaker leads. Pacing Clin Electrophysiol. 2006. 29:852–857.5. Fyke FE 3rd. Simultaneous insulation deterioration associated with side-by-side subclavian placement of two polyurethane leads. Pacing Clin Electrophysiol. 1988. 11:1571–1574.6. Fyke FE 3rd. Infraclavicular lead failure: tarnish on a golden route. Pacing Clin Electrophysiol. 1993. 16:373–376.7. Kiviniemi MS, Pirnes MA, Eranen HJ, Kettunen RV, Hartikainen JE. Complications related to permanent pacemaker therapy. Pacing Clin Electrophysiol. 1999. 22:711–720.8. Mathur G, Stables RH, Heaven D, Ingram A, Sutton R. Permanent pacemaker implantation via the femorla vein: an alternative in cases with contraindications to the pectoral approach. Europace. 2001. 3:56–59.9. Ellestad MH, French J. Iliac vein approach to permanent pacemaker implantation. Pacing Clin Electrophysiol. 1989. 12:1030–1033.10. Michaelsson M, Riesenfeld T, Jonzon A. Natural history of congenital complete atrioventricular block. Pacing Clin Electrophysiol. 1997. 20:2098–2101.11. Kim WJ, Shim JJ, Kim HS, et al. Familial sick sinus syndrome. Korean Circ J. 2003. 33:1155–1160.12. Greenberg SM, Epstein AE, Deering T, et al. A comparison of ICD implantations in the United States versus Italy. Pacing Clin Electrophysiol. 2007. 30:1. S143–S146.13. Kim DH, Kim SY, Lee KH, et al. Follow-up of a group of patients with automatic implantable defibrillator. Korean Circ J. 2005. 35:69–83.14. Shefer A, Lewis BS, Gang ES. The retropectoral transaxillary permanent pacemaker: description of a technique for percutaneous implantation of an "invisible" device. Pacing Clin Electrophysiol. 1996. 19:1646–1651.15. Belott PH, Bucko D. Inframammary pulse generator placement for maximizing cosmetic effect. Pacing Clin Electrophysiol. 1983. 6:1241–1244.16. Roelke M, Jackson G, Harthorne JW. Submammary pacemaker implantation: a unique tunneling technique. Pacing Clin Electrophysiol. 1994. 17:1793–1796.17. Foster AH. Technique for implantation of cardioverter defibrillators in the subpectoral position. Ann Thorac Surg. 1995. 59:764–767.18. Sekiguchi M, Yazaki Y, Isobe M, Hiroe M. Cardiac sarcoidosis: diagnostic, prognostic, and therapeutic considerations. Cardiovasc Drugs Ther. 1996. 10:495–510.19. Chapelon-Abric C, de Zuttere D, Duhaut P, et al. Cardiac sarcoidosis: a retrospective study of 41 cases. Medicine. 2004. 83:315–334.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sensory Loss of Upper Inner Arm and Nipple after Transaxillary and Periareolar Augmentation Mammaplasty - MDbP204
- A Case of Pacemaker Implantation after Balloon Venoplasty on Innominate Vein Stenosis
- Results of Permanent Cardiac Pacemaker Implantation in Ewha Womans University Mokdong Hospital
- Early Detection of Perforation of the Right Ventricle by a Permanent Pacemaker Lead
- A Case Report of Rare Complications after Epicardial Permanent Pacemaker Implantation in an Infant: Airway Compression, Skin Necrosis, and Bowel Perforation
