A Case of Colloid Carcinoma Arising in Association with Intraductal Papillary Neoplasm of the Liver
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University Hospital, Daejeon, Korea. mhs1357@cnuh.co.kr
- KMID: 1773077
- DOI: http://doi.org/10.4166/kjg.2012.60.6.386
Abstract
- Colloid carcinoma of the liver is very rare, and its clinicopathologic features have not been well characterized yet. We describe herein a case of colloid carcinoma of the liver. Imaging revealed a lobulated mass, measuring 12 cm in diameter at the right lobe of the liver with direct invasion of adjacent peripheral intrahepatic bile ducts. Right hemihepatectomy of the liver was performed according to the possibility of the tumor's malignant behavior. Histopathological examination of the specimen revealed large extracelluar stromal mucin pools containing floating cuboidal to columnar neoplastic cells without ovarian-like stroma. This case seemed to be colloid carcinoma arising in association with intraductal papillary neoplasm of the liver.
Keyword
MeSH Terms
Figure
-
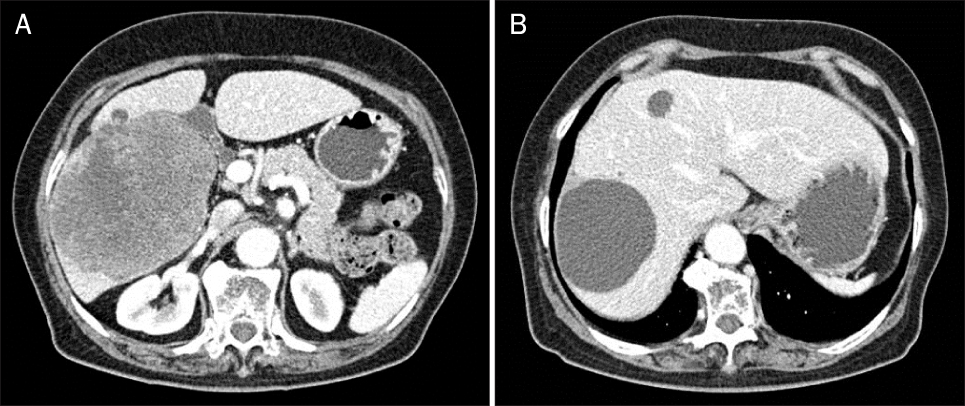
Fig. 1 CT revealed a lobulated mass measuring 12.0 cm in diameter at the right lobe of the liver (A) and variable sized simple cysts, largest one at the right posterosuperior segment measuring about 7.4 cm (B).

Fig. 2 MRI revealed a low attenuating mass as high in the T2-weighted image with mild enhancement of numerous septa and irregular large cystic portion.
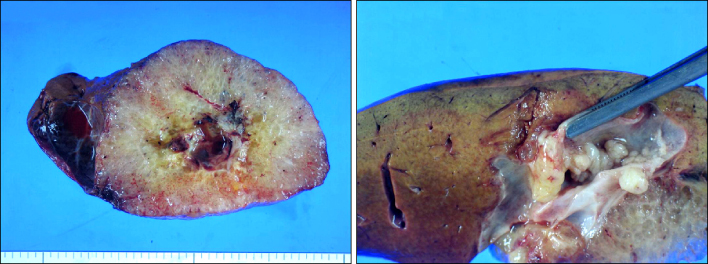
Fig. 3 The gross appearance of the resected specimen showed well demarcated solid mucoid mass without capsule, measuring 13.0×12.0×10.0 cm in size with multiple small papillary nodules in the lumen of the bile duct.
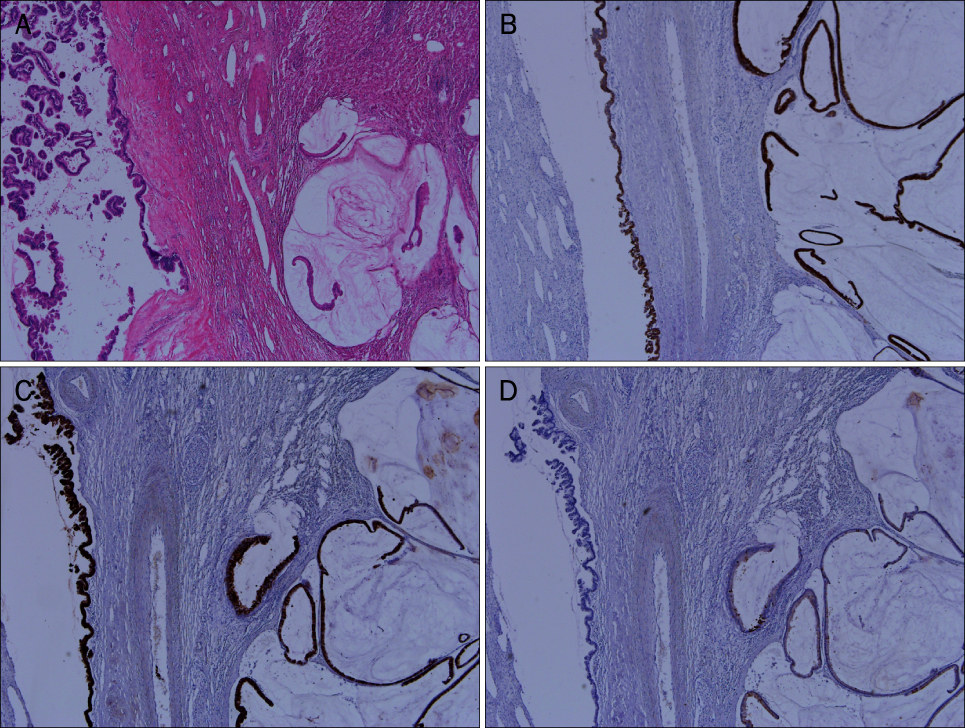
Fig. 4 Microscopic findings (×40). (A) Intraductal papillary neoplasm (IPN; left side) and colloid carcinoma (CC; right side) (H&E, ×40). (B) IPN and CC showed mucin core protein (MUC) 6 positive (MUC6 immunohistochemical stain, ×40). (C) IPN and CC showed MUC5AC positive (MUC5AC immunohistochemical stain, ×40). (D) IPN and CC showed MUC2 negative (MUC2 immunohistochemical stain, ×40).
Reference
-
1. Adsay NV, Pierson C, Sarkar F, et al. Colloid (mucinous noncystic) carcinoma of the pancreas. Am J Surg Pathol. 2001. 25:26–42.2. Silverberg SG, Kay S, Chitale AR, Levitt SH. Colloid carcinoma of the breast. Am J Clin Pathol. 1971. 55:355–363.3. Minsky BD, Mies C, Rich TA, Recht A, Chaffey JT. Colloid carcinoma of the colon and rectum. Cancer. 1987. 60:3103–3112.4. Sadler TW. Langman's medical embryology. 2006. 10th ed. Philadelphia: Williams & Wilkins.5. Rocha FG, Lee H, Katabi N, et al. Intraductal papillary neoplasm of the bile duct: A biliary equivalent to intraductal papillary mucinous neoplasm of the pancreas? Hepatology. 2012. 56:1352–1360.6. Shibahara H, Tamada S, Goto M, et al. Pathologic features of mucin-producing bile duct tumors: two histopathologic categories as counterparts of pancreatic intraductal papillary-mucinous neoplasms. Am J Surg Pathol. 2004. 28:327–338.7. Nakanishi Y, Zen Y, Kondo S, Itoh T, Itatsu K, Nakanuma Y. Expression of cell cycle-related molecules in biliary premalignant lesions: biliary intraepithelial neoplasia and biliary intraductal papillary neoplasm. Hum Pathol. 2008. 39:1153–1161.8. Kim KM, Lee JK, Shin JU, et al. Clinicopathologic features of intraductal papillary neoplasm of the bile duct according to histologic subtype. Am J Gastroenterol. 2012. 107:118–125.9. Nakanuma Y, Sasaki M, Ishikawa A, Tsui W, Chen TC, Huang SF. Biliary papillary neoplasm of the liver. Histol Histopathol. 2002. 17:851–861.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous Encapsulated Papillary Carcinoma and Invasive Ductal Carcinoma Arising from Intraductal Papilloma in the Same Breast: A Case Report
- Intraductal Papillary Mucinous Tumor Simultaneously Involving the Liver and Pancreas: A Case Report
- A Case of Intraductal Papillary Mucinous Neoplasm Arising from Santorini's Duct in a Patient with Complete Type of Pancreas Divisum
- A Case of Papillary Carcinoma in Thyroglossal Duct Cyst with Mandibular Invasion
- Characterization of Intraductal Papillary Neoplasm of the Bile Duct with Respect to the Histopathologic Similarities to Pancreatic Intraductal Papillary Mucinous Neoplasm
