Prenatal Ultrasound Findings of Fetal Neoplasms
- Affiliations
-
- 1Department of Radiology, Samsung Cheil Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. radjycho@samsung.co.kr
- 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1758449
- DOI: http://doi.org/10.3348/kjr.2002.3.1.64
Abstract
- A variety of neoplasms can develop in each tetal organ. Most fetal neoplasms can be detected by careful prenatal ultrasonographic examination. Some neoplosms show specific ultrasonographic findings suggesting the differential diagnosis, but others do not. Knowledge of the presence of a neoplasm in the fetus may alter the prenatal management of a pregnancy and the mode of delivery, and facilitates immediate postnatal treatment. During the last five years, we experienced 32 cases of fetal neoplasms in a variety of organs. We describe their typical ultrasonographic findings with correlating postnatal CT, MRI, and pathologic findings.
Keyword
MeSH Terms
Figure
-

Fig. 1 Prenatal ultrasonographic findings of fetal brain teratoma in a 35-week fetus. A, B. Axial and coronal ultrasonographic images of the fetal head show that a large mass of mixed echogenicity (arrows) has replaced normal brain structures.
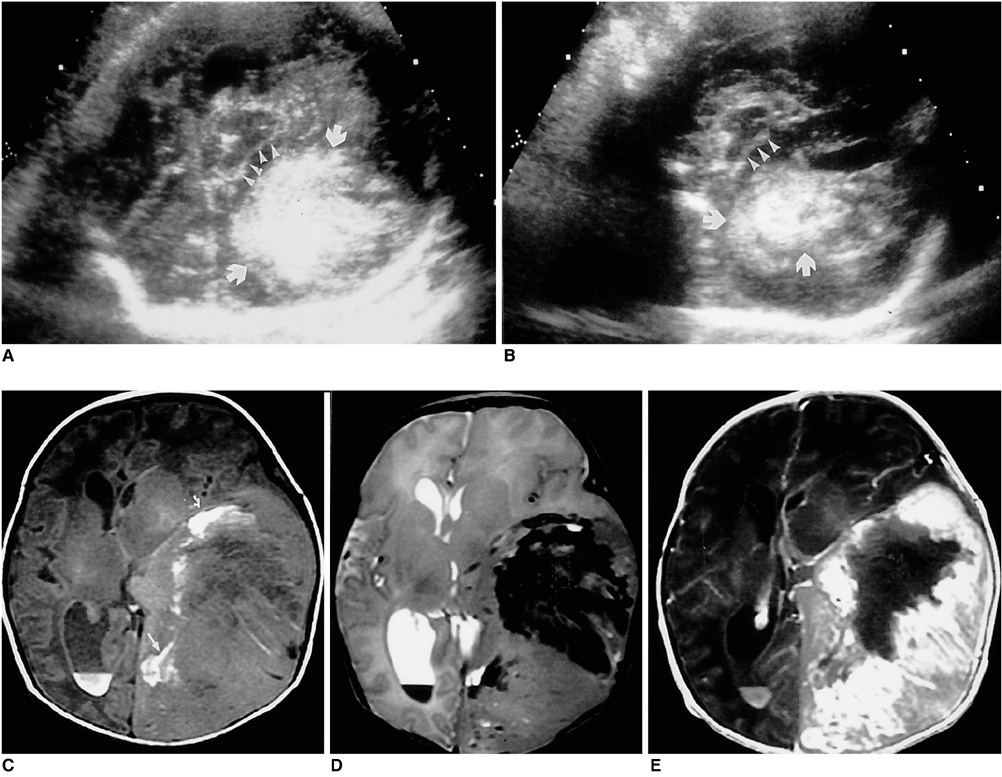
Fig. 2 Prenatal ultrasonographic and postnatal MR findings of fetal glioblastoma. A, B. Axial and coronal ultrasonographic images of the fetal head depict a large mass of mixed echogenicity (arrows) at the left side of cerebral hemisphere. The margin of the mass is ill defined. The midline of the brain (arrowheads) has shifted to the right, and the right hemisphere is compressed by the mass. C. T1WI demonstrates a large ill-defined mass in the left cerebral hemisphere. The observed high signal intensity (small arrows) is due to intratumoral hemorrhage. D. T2WI reveals heterogeneous signal intensity due to hemorrhage and necrosis. E. Contrast-enhanced T1WI shows bright enhancement, with central necrosis.
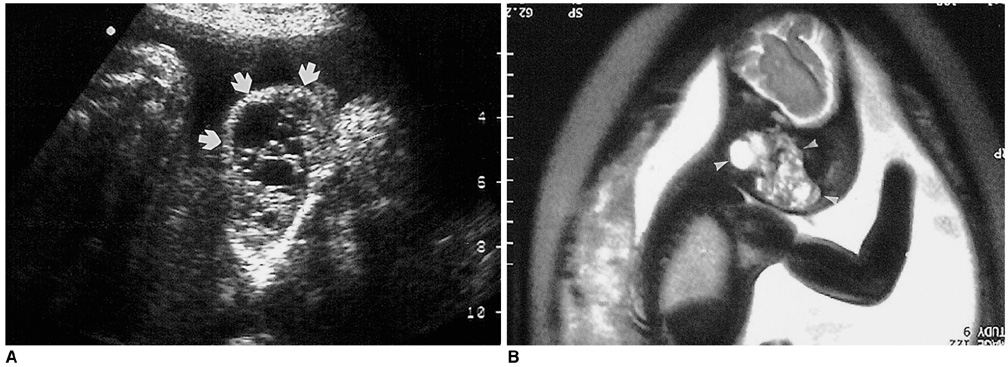
Fig. 3 Prenatal ultrasonographic and MRI findings of a 26-week fetus with bilateral cervical lymphangioma. A. Coronal ultrasonographic image shows multiseptated cystic masses (arrows) at both sides of the fetal neck and chin. B. Sagittal fetal MRI demonstrates a multiseptated cystic mass (arrowheads) at the left side of the fetal neck and chin.
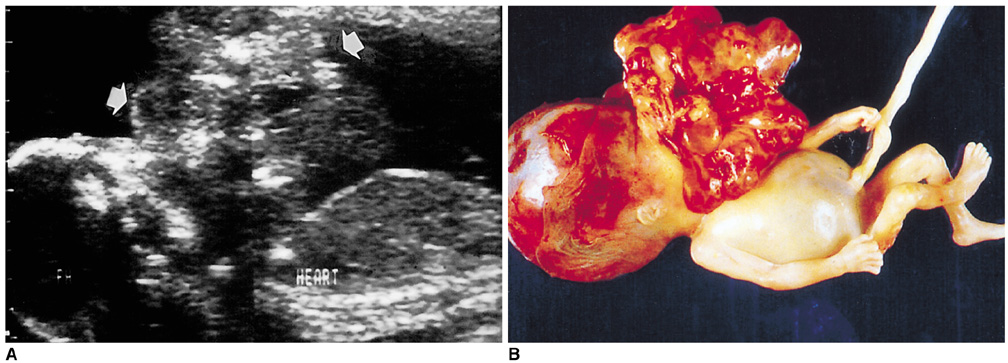
Fig. 4 Prenatal ultrasonographic findings and photograph of a large cervical teratoma. A. Sagittal fetal image shows a large pedunculated mass of mixed echogenicity (arrows) at the anterior aspect of the fetal face and neck. B. Photograph of the fetus shows a large pedunculated mass originating from the oral cavity.

Fig. 5 Prenatal ultrasonographic finding and photograph of a 22-week fetus with a large chest-wall lymphangioma. A. Axial image of the fetal upper abdomen demonstrates a large exophytic mass of mixed echogenicity (solid arrows) in the left chest wall. B. The photograph depicts a large exophytic mass in the left chest wall.

Fig. 6 Prenatal and postnatal ultrasonographic findings of cardiac rhabdomyomas. A. Prenatal ultrasonographic of a 27-week fetus reveals a round echogenic mass (arrow) in the lower portion of the right ventricle. B. Out-tract view of the fetal heart shows thickened interventricular septum and ventricular wall with multifocal increased echogenicities (arrows) suggesting multiple rhabdomyomas. C. Neonatal echocardiography depicts a round echogenic mass (arrows) in the right ventricle. D. Multiple echogenic nodules (arrows) are seen at the interventricular septum and ventricular wall.
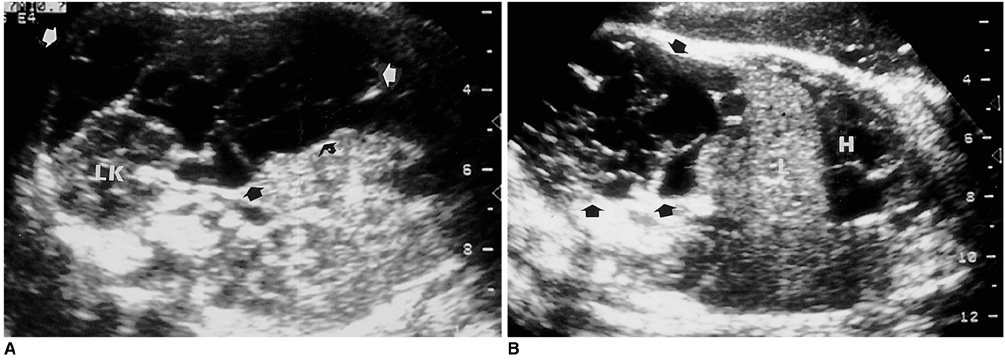
Fig. 7 Prenatal ultrasonographic findings of retroperitoneal lymphangioma in a 32-week fetus. A, B. Axial and coronal images of the fetal abdomen depict a large multiseptated cystic lesion (arrows) in the left retroperitoneal space (LK: left kidney, LV: liver, H: heart).
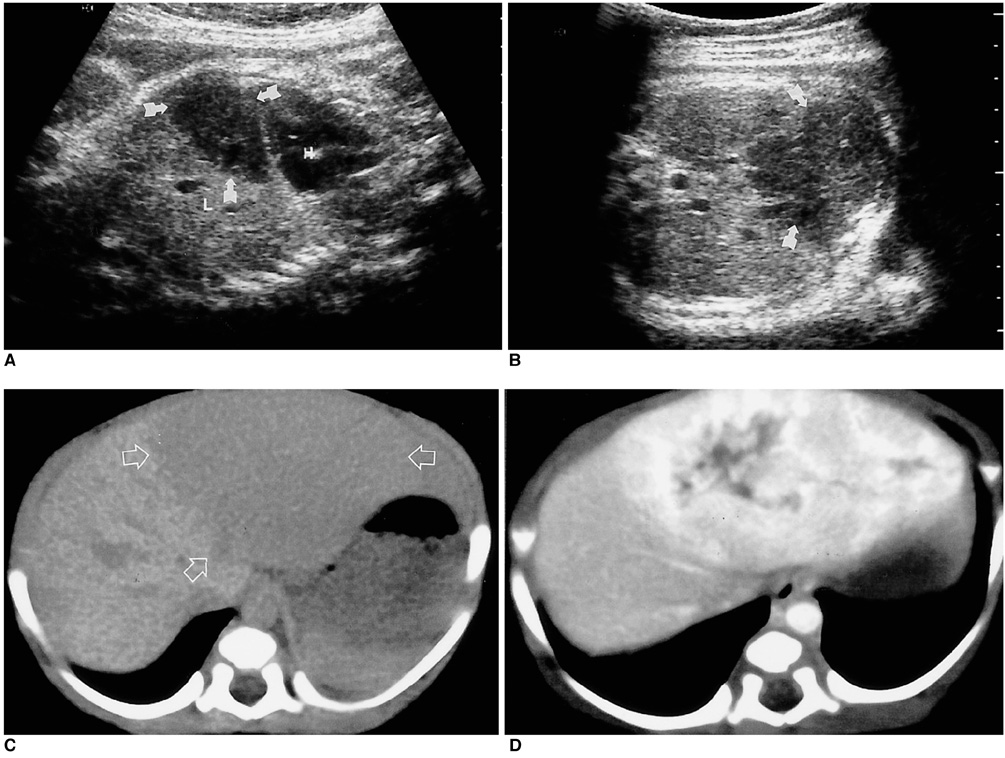
Fig. 8 Prenatal ultrasonographic and postnatal CT findings of hepatocellular adenoma. A, B. Coronal and axial ultrasonographic images of a 33-week fetus reveal a well-defined mass of low echogenicity (arrows) in the left lobe of the fetal liver (L: liver). C. Nonenhanced CT scan depicts a well-demarcated large mass (open arrows) in the left lobe of the liver. D. Contrast-enhanced CT scan demonstrates the early enhancement of the mass. Irregular unenhanced areas suggesting necrosis are apparent.
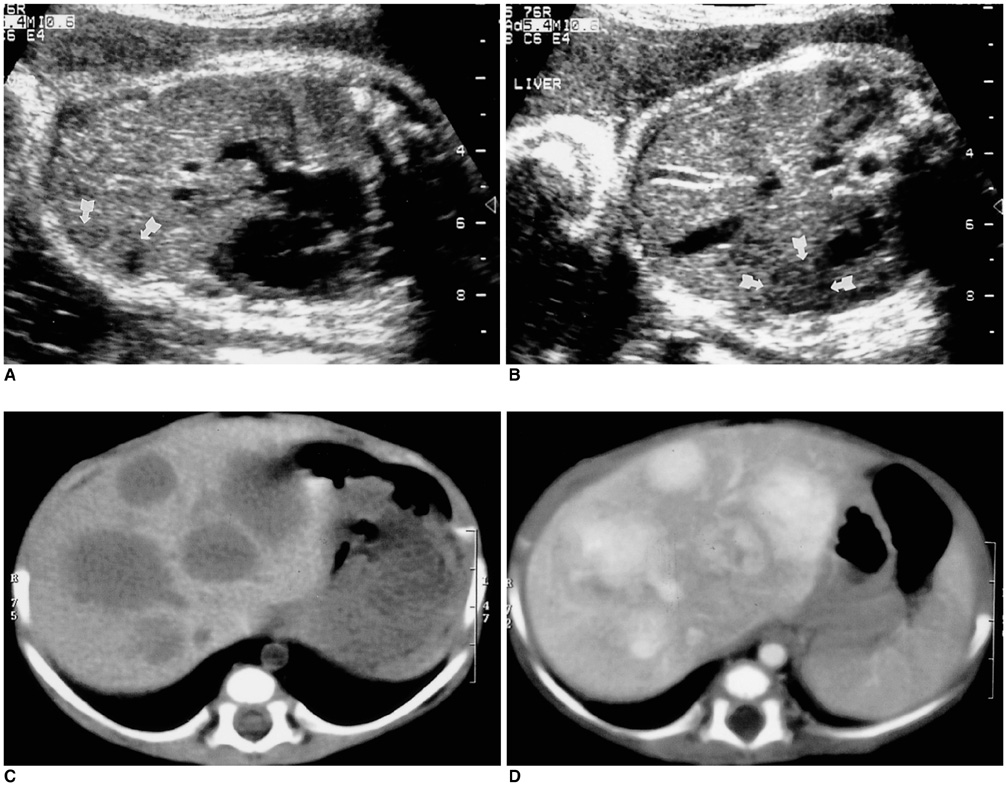
Fig. 9 Prenatal ultrasonographic and postnatal CT findings of multiple hepatic hemangiomas. A, B. Coronal and axial ultrasomographic images of a 31-week fetus depict dilated hepatic veins, probably due to arteriovenous shunt. Ill-defined lesions of low echogenicity (arrows) are seen in the left lobe of the fetal liver, but were not by prenatal ultrasonographic. C. Nonenhanced CT scan shows multiple well-demarcated large masses in the liver. D. Contrast-enhanced CT scan demonstrates strong early enhancement.

Fig. 10 Prenatal ultrasonographic findings of mesoblastic nephroma in a 34-week-old fetus. A. Sagittal image reveals a markedly enlarged right kidney (arrows), with increased echogenicity throughout the entire renal area. The crescent-shaped lesion (☆) occupying the perirenal space is probably due to the tumor extension and hematoma. B. Power Doppler ultrasonographic image shows a vessel penetrating the renal capsule as far as the perirenal space.

Fig. 11 Prenatal ultrasonographic and postnatal CT findings of neuroblastoma. A, B. Axial and coronal ultrasonographic images of a 32-week fetus depict a round echogenic mass (arrows) in the left suprarenal paraspinal area. The mass abuts to the right adrenal gland (arrowheads). C. Nonenhanced CT image demonstrates a small solid mass (arrow) in the supero-anterior portion of the left kidney. D. Contrast-enhanced CT image shows mild enhancement of the mass (arrow).
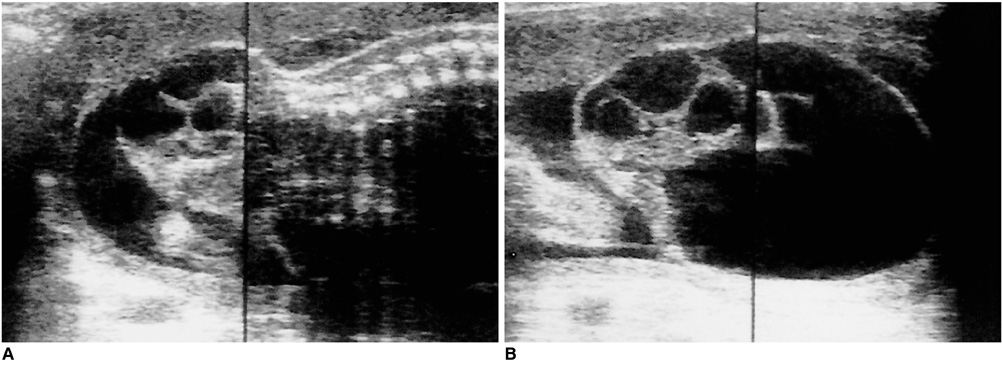
Fig. 12 Typical ultrasonographic findings of sacrococcygeal teratoma in a 33-week fetus. A. Sagittal image reveals an exophytic solid and cystic mass, the intrapelvic extent of which is not well defined, in the perineal area. B. Axial image of the same mass depict its cystic and solid components.
Reference
-
1. Lipman SP, Pretorius DH, Rumack CM, et al. Fetal intracranial teratoma; US diagnosis of three cases and a review of the literature. Radiology. 1985. 157:491–494.2. Teal LN, Angtauco TL, Jimenez JF, Quirk JG. Fetal teratomas: antenatal diagnosis and clinical management. J Clin Ultrasound. 1988. 16:329–336.3. Buetow PC, Smirniotopoulos JG, Done S. Congenital brain tumors: a review of 45 cases. AJR. 1990. 155:587–593.4. Garaghty AV, Knott PD, Hanna HM. Prenatal diagnosis of fetal glioblastma multiforme. Prenat Diagn. 1989. 9:613–616.5. Sabet LM. Congenital glioblastoma multiforme associated with congestive heart failure. Arch Pathol Lab Med. 1982. 106:31–34.6. Zadvinskis DP, Benson MT, Kerr HH, et al. Congenital malformations of the cervicothoracic lymphatic system: embryology and pathogenesis. Radiographics. 1992. 12:1175–1189.7. Pui MH, Li ZP, Chen W, Chen JH. Lymphangioma: imaging diagnosis. Australasian Radiology. 1997. 41:324–328.8. Rempen A, Feige A. Differential diagnosis of sonographically detected tumors in the fetal cervical region. Europ J Obstet Gynecol Reprod Biol. 1985. 20:89–105.9. Kerner B, Flaum E, Mathews H, et al. Cervical teratoma: prenatal diagnosis and long-term follow-up. Prenat Diagn. 1998. 18:51–59.10. Rosenfeld CR, Coln CD, Duenhoelter JH. Fetal cervical teratoma as a cause of polyhydramnios. Pediatrics. 1979. 64:176–179.11. Holley D, Martin G, Brenner J, et al. Diagnosis and management of fetal cardiac tumors: A multicenter experience and review of published reports. J Am Coll Cardiol. 1995. 26:516–520.12. Giacoia GP. Fetal rhabdomyoma: a prenatal echocardiographic marker of tuberous sclerosis. Am J Perinatol. 1992. 9:111–114.13. Green KW, Bros-Koefoed R, Pollack P, et al. Antepartum diagnosis and management of multiple fetal cardiac tumors. J Ultrasound Med. 1991. 10:697–699.14. Takiff H, Calabria R, Yin L, Stabile BE. Mesenteric cysts and intra-abdominal cystic lymphangiomas. Arch Surg. 1985. 120:1266–1269.15. Stoupos C, Ros PR, Abbit PL, Burton SS, Gauger J. Bubbles in the belly: Imaging of cystic mesenteric or omental masses. Radiographics. 1994. 14:729–737.16. de Perrot M, Rostan O, Morel P, Le Coultre C. Abdominal lymphangioma in adults and children. Br J Surg. 1998. 85:395–397.17. Takano H, Smith WL. Gastrointestinal tumors of childhood. Radiol Clin North Am. 1997. 35:1367–1389.18. Chung KY, Mayo-Smith WW, Saini S, et al. Hepatocellular adenoma: MR imaging features with pathologic correlation. AJR. 1995. 165:303–308.19. Dreyfus M, Baldauf JJ, Dadoun K, Becmeur F, Berrut F, Ritter J. Prenatal diagnosis of hepatic hemangioma. Fetal Diagn Ther. 1996. 11:57–60.20. Chuileannain FN, Rowlands S, Sampson A. Ultrasonographic appearances of fetal hepatic hemangioma. J Ultrasound Med. 1999. 18:379–381.21. Fishman SJ, Mulliken JB. Hemangiomas and vascular malformations of infancy and childhood. Pediatr Clin North Am. 1993. 40(6):1177–1200.22. Irsutti M, Puget C, Baunin C, Duga I, Sarramon MF, Guitard J. Mesoblastic nephroma: prenatal ultrasonographic and MRI features. Pediatr Radiol. 2000. 30:147–150.23. Dimaggio HD, Farrell EE, Sholl J, et al. Congenital mesoblastic nephroma: prenatal ultrasonic findings and surgical excision in a very-low-birth-weight infant. J Clin Ultrasound. 1985. 13:506–508.24. Geirsson RT, Ricketts NE, Taylor DJ, et al. Prenatal appearance of a mesoblastic nephroma associated with polyhydroamnios. J Clin Ultrasound. 1985. 13:488–490.25. Bader JL, Miller RW. US cancer incidence and mortality in the first year of life. Am J Dis Child. 1979. 133:157–161.26. Ferraro EM, Fakhry J, Aruny J. Prenatal adrenal neuroblastoma: A case report with review of the literature. J Ultrasound Med. 1988. 7:275–278.27. Granata C, Fagnani AM, Gambini C, et al. Features and outcome of neuroblastoma detected before birth. J Pediatr Surg. 2000. 35:88–91.28. Sheth S, Nussbaum AR, Sanders RC, Hamper UM, Davison AJ. Prenatal diagnosis of sacrococcygeal teratoma: Sonographic-pathologic correlation. Radiology. 1988. 169:131–136.29. Tongsong T, Wanapirak C, Piyamongkol W, Sudasana J. Prenatal sonographic features of sacrococcygeal teratoma. Int J Gynaecol Obstet. 1999. 67:95–101.30. Bond SJ, Harrison MR, Schmidt KG, et al. Death due to high-output failure in fetal sacrococcygeal teratoma. J Pediatr Surg. 1990. 25:1287–1291.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prenatal Ultrasonographic Diagnosis of Frequent Congenital Fetal Anomalies
- Prenatal Ultrasound of Horseshoe Kidney: A Case Report
- Recent Trends in Prenatal Diagnosis of Fetal Malformations
- Prenatal ultrasonography of craniofacial abnormalities
- Prenatal Detection of a Congenital Pancreatic Cyst by Ultrasound
