Multi-Detector CT Findings of Palpable Chest Wall Masses in Children: A Pictorial Essay
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital, Cheonan, Korea. ytokim@schmc.ac.kr
- 2Department of Radiology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea.
- KMID: 1748462
- DOI: http://doi.org/10.3348/jksr.2013.68.3.261
Abstract
- A wide variety of diseases manifest as palpable chest wall masses in children. These include normal variation, congenital anomalies, trauma, infection, axillary lymphadenopathies, soft tissue tumors and bone tumors. Given that most of these diseases are associated with chest wall deformity, diagnosis is difficult by physical examination or ultrasonography alone. However, multi-detector CT with three dimensional reconstruction is useful in the characterization and differential diagnosis of palpable chest wall lesions. In this article, we review the spectrum of palpable chest wall diseases and illustrate their multi-detector CT presentation.
MeSH Terms
Figure
-

Fig. 1 Anterior convexity of the right costal cartilage in a 10-year-old girl clinically diagnosed with rib tumor. Axial CT scan showing asymmetrically protruding right anterior chest wall (arrow).

Fig. 2 Bony irregularity of the rib in a 4-year-old boy who presented with a palpable chest wall mass. A, B. Axial (A) and three dimensional (B) images revealing irregular bony protrusion (arrow) in the anterior portion of the left rib.
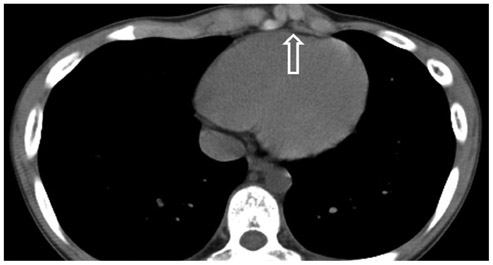
Fig. 3 Asymmetrically protruding costal cartilage in a 12-year-old boy who visited the hospital for evaluation of chest wall deformity. Axial CT scan illustrating asymmetrically protruding costal cartilage (open arrow) in left anterior chest wall.

Fig. 4 Asymmetric thoracic cavity due to protruding left chest wall in a 13-year-old boy with a 2-3 year history of palpable mass in the left chest wall. Axial CT scan shows that the left thoracic cavity is asymmetrically larger than the right thoracic cavity.

Fig. 5 Focal lipomatosis in a 12-year-old girl presenting with a posterior chest wall lump. Pre-contrast axial CT scan obtained with patient in prone position demonstrates prominent fat deposition (arrowheads) in the midline of the posterior chest wall and no evident mass.
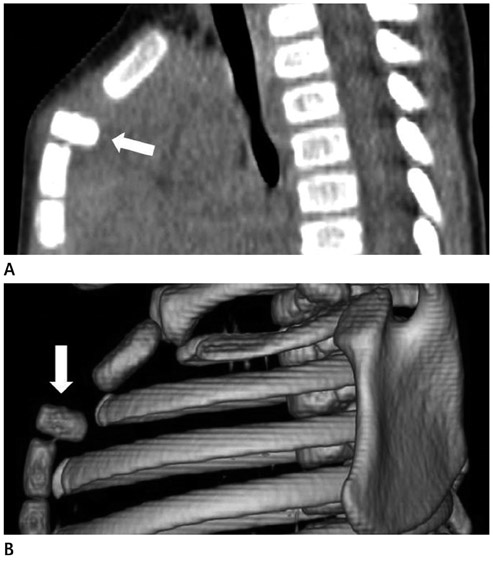
Fig. 6 Sternal segmental dislocation in a 4-year-old boy presenting with seven-day history of chest wall lump. A, B. Reformatted (A) and three dimensional (B) images revealing transverse oriented first segment (arrow) of the sternal body.
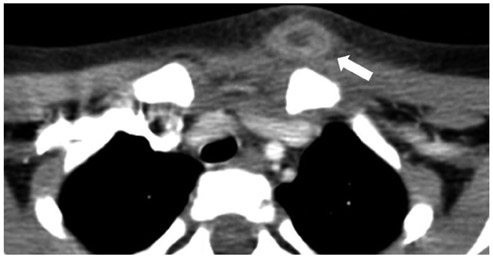
Fig. 7 An infected epidermal cyst in a 3-year-old boy who was born with a palpable mass on the left chest wall. Axial CT scan illustrating a protruded left chest wall due to abscess formation (arrow). Excisional biopsy confirmed the lesion as an epidermal cyst with inflammation.

Fig. 8 Chest wall abscesses in a 2-month-old girl. A. Reformatted coronal image showing one abscess (arrows) in the right chest wall, and a further abscess (arrowheads) in the left supraclavicular area. Staphylococcus aureus was isolated from the aspirated fluid in the abscess cavity, obtained by ultrasound-guided aspiration. B. Chest radiograph 20 days later demonstrating permeative bone destruction (open arrowheads) of the left clavicle, suggesting bone involvement of the surrounding abscess. C. Axial bone setting CT scan clearly showing permeative bone destruction (open arrow) of the left clavicle, with superior image quality to chest radiograph.
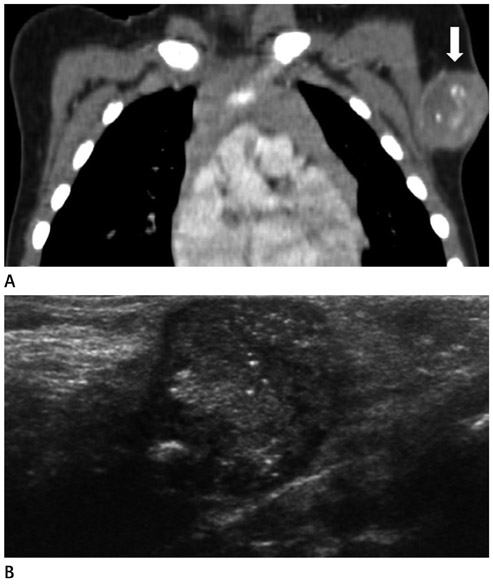
Fig. 9 BCG lymphadenitis in a 22-month-old boy who presented with persistent axillary mass of 7 months' duration. A. Coronal reformatted post-contrast image demonstrating a well-marginated, rim-enhancing mass with multiple internal calcifications (arrow) in the left axilla. This was confirmed as chronic granulomatous inflammation by excision. B. USG showing a circumscribed oval hypoechoic mass with internal calcifications in the left axilla. Note.-BCG = Bacillus Calmette-Guerin, USG = ultrasonography
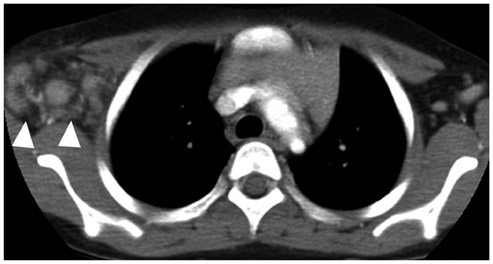
Fig. 10 Acute axillary lymphadenitis in a 6-year-old girl presenting with a two-week history of palpable, growing mass with pain and fever on the right axilla. Axial CT scan illustrates enlarged lymph nodes (arrowheads) with fat infiltration in the right axillary area.
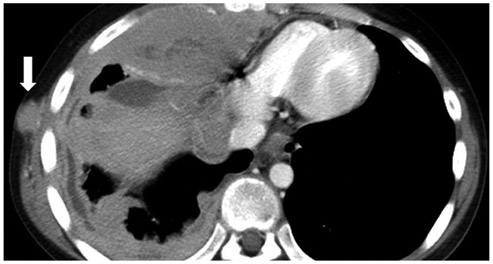
Fig. 11 Burkitt lymphoma in a 12-year-old boy, as diagnosed through biopsy of the abdominal mass. Axial CT scan showing an enhancing mass (arrow) in the right chest wall, and circumferential extensive pleural masses, suggesting a tumor implantation in the chest wall caused by tube thoracoplasty.

Fig. 12 Neurofibromatosis in a 12-year-old boy who had a palpable lesion in the right posterior chest wall. Axial CT scan revealing plexiform neurofibromatosis (open arrowheads) in the right lower chest wall.

Fig. 13 Infantile hemangioma in a 11-year-old boy admitted for a palpable mass four years ago. A. Post-contrast axial CT scan (arterial phase) illustrating a lobulated mass (open arrow) without definite enhancement in the left anterior chest wall. B. Post-contrast axial CT scan (delayed phase) showing diffuse homogenous enhancing mass (open arrow) in the left anterior chest wall.
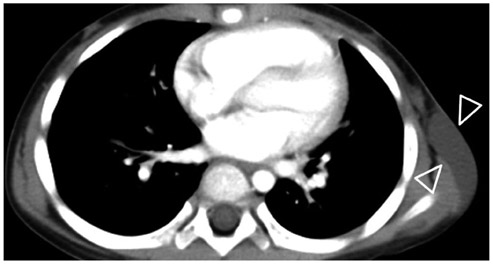
Fig. 14 Lymphatic malformation in a 3-year-old girl who had showed a palpable mass on the left axilla one year before. She visited the hospital due to increasing mass size accompanied by pain. Post-contrast axial scan shows a cystic mass (open arrowheads) with no enhancing wall and a soft tissue mass in the left lateral chest wall.
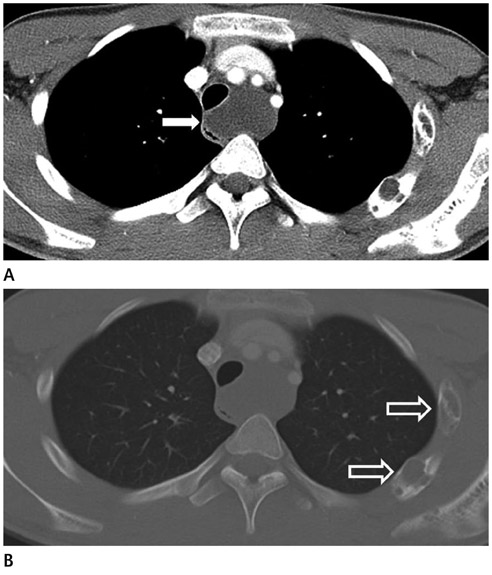
Fig. 15 Lymphangiomatosis in a 16-year-old boy. A, B. Axial mediastinal and bone setting CT scan revealing a homogenous non-enhancing low density mass in the mediastinum (arrow) and expansile osteolytic lesions on the left side of the ribs (open arrows).

Fig. 16 Lipoblastoma in a 9-month-old girl who was referred with an incidentally palpable mass. A, B. Pre-contrast CT scan demonstrates a well-marginated fatty mass with inhomogeneous soft tissue lesion (arrow) in the right anterior chest wall.
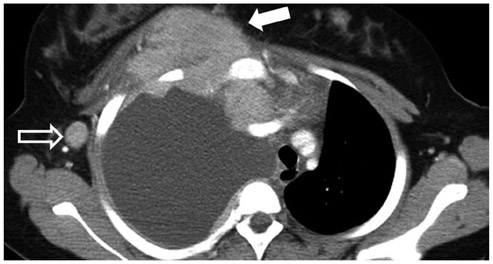
Fig. 17 Rhabdomyosarcoma in a 14-year-old boy who presented with one-week history of dyspnea, tachypnea and swelling of the chest wall. Axial CT scan demonstrating right anterior mediastinal and chest wall masses (arrow), and right axillary lymphadenopathy (open arrow). Note the right pleural effusion with enhancing pleural nodules and thickening.
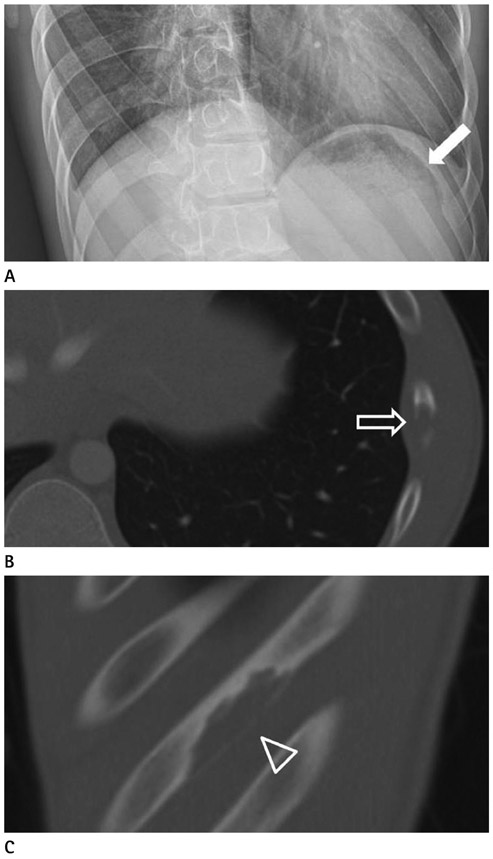
Fig. 18 Langerhans cell histiocytosis in a 16-year-old boy. A. Rib radiograph showing an eccentric osteolytic lesion (arrow) in the left 8th rib. B, C. Axial and sagittal bone setting CT scan demonstrating the eccentric osteolytic lesion (open arrow and open arrowhead) along the long axis of the left 8th rib.

Fig. 19 Fibrous dysplasia in a 18-year-old boy. Axial CT scan with bone setting demonstrating an expansile osteolytic lesion with cortical thinning and endosteal scalloping (arrow) in the left 4th rib.
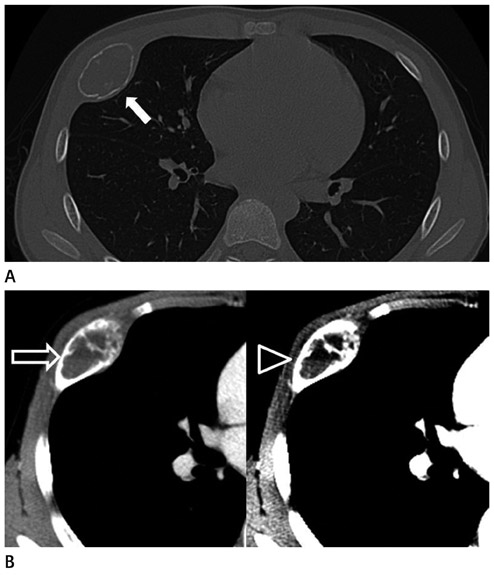
Fig. 20 Aneurysmal bone cyst in a 13-year-old boy who presented with a palpable mass on the right chest wall one week ago. A, B. Axial CT scans illustrating an expansile bone tumor (arrow) with fluid-fluid level (open arrow) in the anterior portion of the right rib. The image with a narrow window width shows the fluid-fluid level more clearly (open arrowhead).
Reference
-
1. Donnelly LF, Frush DP. Abnormalities of the chest wall in pediatric patients. AJR Am J Roentgenol. 1999. 173:1595–1601.2. Jeung MY, Gangi A, Gasser B, Vasilescu C, Massard G, Wihlm JM, et al. Imaging of chest wall disorders. Radiographics. 1999. 19:617–637.3. Donnelly LF. Use of three-dimensional reconstructed helical CT images in recognition and communication of chest wall anomalies in children. AJR Am J Roentgenol. 2001. 177:441–445.4. Wong KS, Hung IJ, Wang CR, Lien R. Thoracic wall lesions in children. Pediatr Pulmonol. 2004. 37:257–263.5. Pawar RV, Blacksin MF. Traumatic sternal segment dislocation in a 19-month-old. Emerg Radiol. 2007. 14:435–437.6. Kim DY, Lee SW, Hwang JY. Ultrasonographic features of BCG lymphadenitis. J Korean Radiol Soc. 2005. 52:31–36.7. Subhawong TK, Fishman EK, Swart JE, Carrino JA, Attar S, Fayad LM. Soft-tissue masses and masslike conditions: what does CT add to diagnosis and management? AJR Am J Roentgenol. 2010. 194:1559–1567.8. Inampudi P, Jacobson JA, Fessell DP, Carlos RC, Patel SV, Delaney-Sathy LO, et al. Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Radiology. 2004. 233:763–767.9. Nield LS, Kamat D. Lymphadenopathy in children: when and how to evaluate. Clin Pediatr (Phila). 2004. 43:25–33.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multi-Detector CT Findings of Typical and Atypical Appendicitis: A Pictorial Essay
- Multi-Slice Spiral CT of Living-Related Liver Transplantation in Children: Pictorial Essay
- Congenital Anomalies of the Coronary Sinus: A Pictorial Essay
- CT Findings of Foreign Bodies in the Chest: A Pictorial Essay
- Azygos System on Multi-Detector Computed Tomography: Pictorial Essay
