Gap Balancing vs. Measured Resection Technique in Total Knee Arthroplasty
- Affiliations
-
- 1Orthopaedic Institute of Southern Illinois, Herrin, IL, USA.
- 2Colorado Joint Replacement, Denver, CO, USA. kendallslutzky@centura.org
- 3Department of Biomedical Engineering, University of Tennessee, Knoxville, TN, USA.
- 4Department of Bioengineering, University of Denver, Denver, CO, USA.
- 5Department of Orthopaedics, University of Colorado School of Medicine, Denver, CO, USA.
- KMID: 1737625
- DOI: http://doi.org/10.4055/cios.2014.6.1.1
Abstract
- A goal of total knee arthroplasty is to obtain symmetric and balanced flexion and extension gaps. Controversy exists regarding the best surgical technique to utilize to obtain gap balance. Some favor the use of a measured resection technique in which bone landmarks, such as the transepicondylar, the anterior-posterior, or the posterior condylar axes are used to determine proper femoral component rotation and subsequent gap balance. Others favor a gap balancing technique in which the femoral component is positioned parallel to the resected proximal tibia with each collateral ligament equally tensioned to obtain a rectangular flexion gap. Two scientific studies have been performed comparing the two surgical techniques. The first utilized computer navigation and demonstrated a balanced and rectangular flexion gap was obtained much more frequently with use of a gap balanced technique. The second utilized in vivo video fluoroscopy and demonstrated a much high incidence of femoral condylar lift-off (instability) when a measured resection technique was used. In summary, the authors believe gap balancing techniques provide superior gap balance and function following total knee arthroplasty.
MeSH Terms
Figure
-

Fig. 1 Intraoperative photograph of a flexion gap tensioning jig placed into the flexion gap, tensioning the gap, and positioned parallel to the transepicondylar axis before the anterior and posterior femoral resections are performed (Courtesy of Robert E. Booth, MD).

Fig. 2 Intraoperative photograph demonstrating a tensioning jig placed into the extension gap with an extramedullary guide used to determine alignment and width of the distal femoral resection (Courtesy of Robert E. Booth, MD).

Fig. 3 (A) Intraoperative photograph demonstrating resection of 4 mm of the posterior aspect of the medial femoral condyle to gain access to posterior compartment osteophytes. (B) Photograph demonstrating how an osteotome with greater curvature allows for easier access to posterior femoral osteophytes than a traditional curved osteotome. (C) Intraoperative photograph demonstrating removal of posterior femoral osteophytes using a curved osteotome.
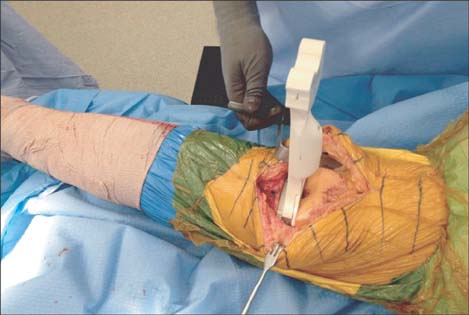
Fig. 4 Intraoperative photograph demonstrating assessment of lower extremity alignment and extension gap balance using a spacer block.
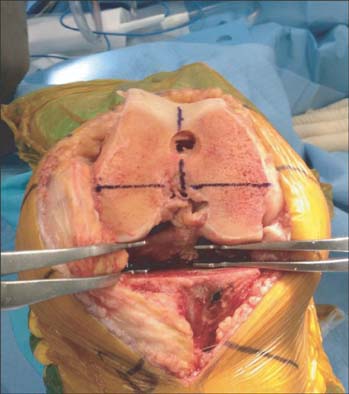
Fig. 5 Intraoperative photograph of the knee at 90 degrees of flexion and the collateral ligaments equally tensioned using laminar spreaders. Note the transepicondylar axis is parallel and anterior-posterior axis is perpendicular to the resected proximal tibia.
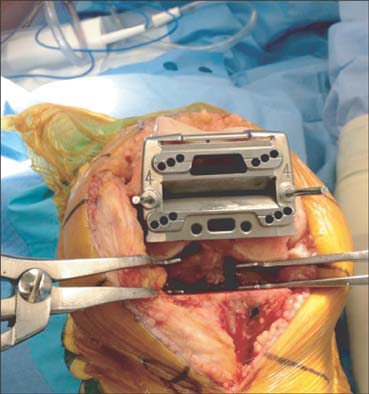
Fig. 6 Intraoperative photograph demonstrating placement of the anteroposterior femoral cutting block parallel to the resected proximal tibia with each collateral ligament tensioned to create a rectangular flexion gap.
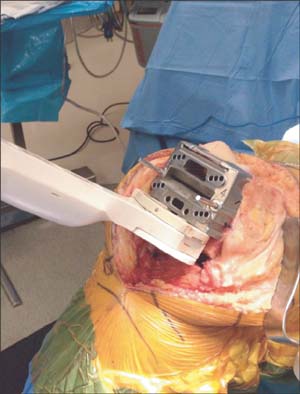
Fig. 7 Intraoperative photograph demonstrating placement of a spacer block (same width as utilized in creation of the extension gap) into the flexion gap to assure appropriate width before performing the anterior and posterior femoral condylar resections.
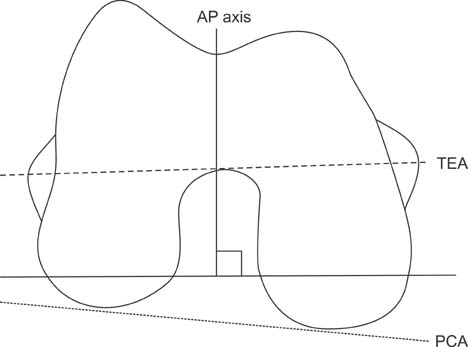
Fig. 8 Diagram demonstrating the transepicondylar (TEA), anterior-posterior (AP), and posterior condylar (PCA) axes.
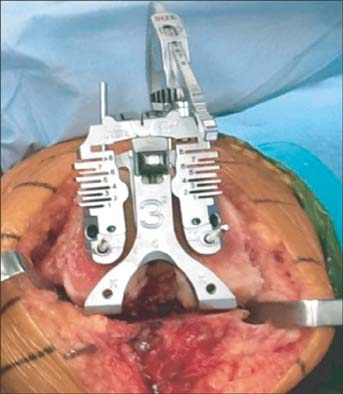
Fig. 9 Intraoperative photograph demonstrating use of a femoral rotational alignment guide applied to the distal femur and aligned along the posterior condylar axis to assure three degrees of external rotation relative to the posterior condylar axis.
Cited by 1 articles
-
Computer-Assisted Navigation in Total Knee Arthroplasty
Hwa-Jae Jeong, Yong-Beom Park, Han-Jun Lee
J Korean Orthop Assoc. 2018;53(6):478-489. doi: 10.4055/jkoa.2018.53.6.478.
Reference
-
1. Laskin RS. Flexion space configuration in total knee arthroplasty. J Arthroplasty. 1995; 10(5):657–660.2. Scuderi GR, Komistek RD, Dennis DA, Insall JN. The impact of femoral component rotational alignment on condylar lift-off. Clin Orthop Relat Res. 2003; (410):148–154.3. Berger RA, Crossett LS, Jacobs JJ, Rubash HE. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res. 1998; (356):144–153.4. Boldt JG, Stiehl JB, Hodler J, Zanetti M, Munzinger U. Femoral component rotation and arthrofibrosis following mobile-bearing total knee arthroplasty. Int Orthop. 2006; 30(5):420–425.5. Incavo SJ, Wild JJ, Coughlin KM, Beynnon BD. Early revision for component malrotation in total knee arthroplasty. Clin Orthop Relat Res. 2007; 458:131–136.6. Romero J, Stahelin T, Binkert C, Pfirrmann C, Hodler J, Kessler O. The clinical consequences of flexion gap asymmetry in total knee arthroplasty. J Arthroplasty. 2007; 22(2):235–240.7. Insall JN, Scott WN. Insall & Scott surgery of the knee. 4th ed. Philadelphia: Church Livingstone/Elsevier;2006.8. Lotke PA, Lonner JH. Knee arthroplasty. 3rd ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins;2009.9. Heesterbeek PJ, Jacobs WC, Wymenga AB. Effects of the balanced gap technique on femoral component rotation in TKA. Clin Orthop Relat Res. 2009; 467(4):1015–1022.10. Dennis DA. Measured resection: an outdated technique in total knee arthroplasty. Orthopedics. 2008; 31(9):940943–944.11. Fehring TK. Rotational malalignment of the femoral component in total knee arthroplasty. Clin Orthop Relat Res. 2000; (380):72–79.12. Katz MA, Beck TD, Silber JS, Seldes RM, Lotke PA. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001; 16(3):301–305.13. Griffin FM, Insall JN, Scuderi GR. Accuracy of soft tissue balancing in total knee arthroplasty. J Arthroplasty. 2000; 15(8):970–973.14. Boldt JG, Stiehl JB, Munzinger U, Beverland D, Keblish PA. Femoral component rotation in mobile-bearing total knee arthroplasty. Knee. 2006; 13(4):284–289.15. Dennis DA, Komistek RD, Kim RH, Sharma A. Gap balancing versus measured resection technique for total knee arthroplasty. Clin Orthop Relat Res. 2010; 468(1):102–107.16. Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS. Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res. 1993; (286):40–47.17. Griffin FM, Math K, Scuderi GR, Insall JN, Poilvache PL. Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty. 2000; 15(3):354–359.18. Poilvache PL, Insall JN, Scuderi GR, Font-Rodriguez DE. Rotational landmarks and sizing of the distal femur in total knee arthroplasty. Clin Orthop Relat Res. 1996; (331):35–46.19. Whiteside LA, Arima J. The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop Relat Res. 1995; (321):168–172.20. Mantas JP, Bloebaum RD, Skedros JG, Hofmann AA. Implications of reference axes used for rotational alignment of the femoral component in primary and revision knee arthroplasty. J Arthroplasty. 1992; 7(4):531–535.21. Schnurr C, Nessler J, Konig DP. Is referencing the posterior condyles sufficient to achieve a rectangular flexion gap in total knee arthroplasty? Int Orthop. 2009; 33(6):1561–1565.22. Aglietti P, Sensi L, Cuomo P, Ciardullo A. Rotational position of femoral and tibial components in TKA using the femoral transepicondylar axis. Clin Orthop Relat Res. 2008; 466(11):2751–2755.23. Diduch DR, Insall JN, Scott WN, Scuderi GR, Font-Rodriguez D. Total knee replacement in young, active patients: long-term follow-up and functional outcome. J Bone Joint Surg Am. 1997; 79(4):575–582.24. Miller MC, Berger RA, Petrella AJ, Karmas A, Rubash HE. Optimizing femoral component rotation in total knee arthroplasty. Clin Orthop Relat Res. 2001; (392):38–45.25. Olcott CW, Scott RD. A comparison of 4 intraoperative methods to determine femoral component rotation during total knee arthroplasty. J Arthroplasty. 2000; 15(1):22–26.26. Insall JN, Scuderi GR, Komistek RD, Math K, Dennis DA, Anderson DT. Correlation between condylar lift-off and femoral component alignment. Clin Orthop Relat Res. 2002; (403):143–152.27. Hatayama K, Terauchi M, Higuchi H, Yanagisawa S, Saito K, Takagishi K. Relationship between femoral component rotation and total knee flexion gap balance on modified axial radiographs. J Arthroplasty. 2011; 26(4):649–653.28. Jerosch J, Peuker E, Philipps B, Filler T. Interindividual reproducibility in perioperative rotational alignment of femoral components in knee prosthetic surgery using the transepicondylar axis. Knee Surg Sports Traumatol Arthrosc. 2002; 10(3):194–197.29. Kinzel V, Ledger M, Shakespeare D. Can the epicondylar axis be defined accurately in total knee arthroplasty? Knee. 2005; 12(4):293–296.30. Yau WP, Chiu KY, Tang WM. How precise is the determination of rotational alignment of the femoral prosthesis in total knee arthroplasty: an in vivo study. J Arthroplasty. 2007; 22(7):1042–1048.31. Siston RA, Patel JJ, Goodman SB, Delp SL, Giori NJ. The variability of femoral rotational alignment in total knee arthroplasty. J Bone Joint Surg Am. 2005; 87(10):2276–2280.32. Benjamin J. Determining femoral component position using CAS and measured resection. Clin Orthop Relat Res. 2008; 466(11):2745–2750.33. Arima J, Whiteside LA, McCarthy DS, White SE. Femoral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee: a technical note. J Bone Joint Surg Am. 1995; 77(9):1331–1334.34. Nagamine R, Miura H, Inoue Y, et al. Reliability of the anteroposterior axis and the posterior condylar axis for determining rotational alignment of the femoral component in total knee arthroplasty. J Orthop Sci. 1998; 3(4):194–198.35. Bottros J, Gad B, Krebs V, Barsoum WK. Gap balancing in total knee arthroplasty. J Arthroplasty. 2006; 21:4 Suppl 1. 11–15.36. Laskin RS, Rieger MA. The surgical technique for performing a total knee replacement arthroplasty. Orthop Clin North Am. 1989; 20(1):31–48.37. Hungerford DS, Krackow KA. Total joint arthroplasty of the knee. Clin Orthop Relat Res. 1985; (192):23–33.38. Pagnano MW, Hanssen AD. Varus tibial joint line obliquity: a potential cause of femoral component malrotation. Clin Orthop Relat Res. 2001; (392):68–74.39. Griffin FM, Insall JN, Scuderi GR. The posterior condylar angle in osteoarthritic knees. J Arthroplasty. 1998; 13(7):812–815.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Quantification of the Effect of Vertical Bone Resection of the Medial Proximal Tibia for Achieving Soft Tissue Balancing in Total Knee Arthroplasty
- Comparative Study of Two Techniques for Ligament Balancing in Total Knee Arthroplasty for Severe Varus Knee: Medial Soft Tissue Release vs. Bony Resection of Proximal Medial Tibia
- Gap Discrepancy in Posterior Cruciate Ligament-Sacrificing Total Knee Joint Arthroplasty
- Polyethylene spinout in the Attune® Cruciate-Retaining Rotating-Platform (CR RP) total knee arthroplasty performed with a cruciate-sacrificing and measuredresection technique
- Effects of a Posterior Cruciate Ligament Resection on the Flexion-Extension Gap in Total Knee Arthroplasty
