Computed Tomography and Magnetic Resonance Images of Adrenocortical Oncocytoma Cases
- Affiliations
-
- 1Department of Radiology, Inje University Haeundae Paik Hospital, Busan, Korea. radyjh@hanmail.net
- 2Department of Radiology, Inje University Busan Paik Hospital, Busan, Korea.
- 3Department of Radiology, Dong-A University Hospital, Busan, Korea.
- KMID: 1734936
- DOI: http://doi.org/10.3346/jkms.2014.29.3.445
Abstract
- We present two cases of adrenocortical oncocytomas that were well-delineated on multi-detector computed tomography and magnetic resonance imaging. The images showed a well-enhanced large mass with multiple stippled calcifications in a 10-yr-old girl who was consulted due to precocious puberty. A well-enhanced solid mass with necrotic components was incidentally noticed in a 54-yr-old man. These lesions were resected and diagnosed as adrenocortical oncocytomas through immunohistochemical studies and electron microscopy. Adrenocortical oncocytomas are rare disease entities, therefore, we report these interesting, rare adrenocortical oncocytomas here with radiologic findings, and discuss differential diagnosis.
MeSH Terms
Figure
-

Fig. 1 Adrenocortical oncocytoma in a 10-yr-old girl (Case 1), abdominal multi-detector CT findings. (A) A well-circumscribed, oval-shaped mass in the left adrenal gland with stippled calcifications on a precontrast scan. (B) Thoroughly heterogeneous enhancement during the 1-min delayed axial scan. (C) On a coronal reconstructed image of B. (D) Enhancement washout in the 15-min delayed scan.

Fig. 2 Adrenocortical oncocytoma in a 10-yr-old girl (Case 1), gross and microscopic findings. (A) The tumor was approximately 6×4 cm, well-encapsulated and dark brown in color, and it consisted of multiple small hemorrhagic vascular lakes with old blood. (B, C) A microscopic examination revealed that the neoplasm was comprised of polygonal cells with abundant eosinophilic cells and granular cytoplasm. A nuclear cellular atypia with enlarged nuclei was identified (B: ×200 HPF, C: ×400 HPF, H&E). (D) By electron microscopy, electron dense inclusions, as well as closely packed mitochondria with Golgi complexes, were found (×400 HFP).
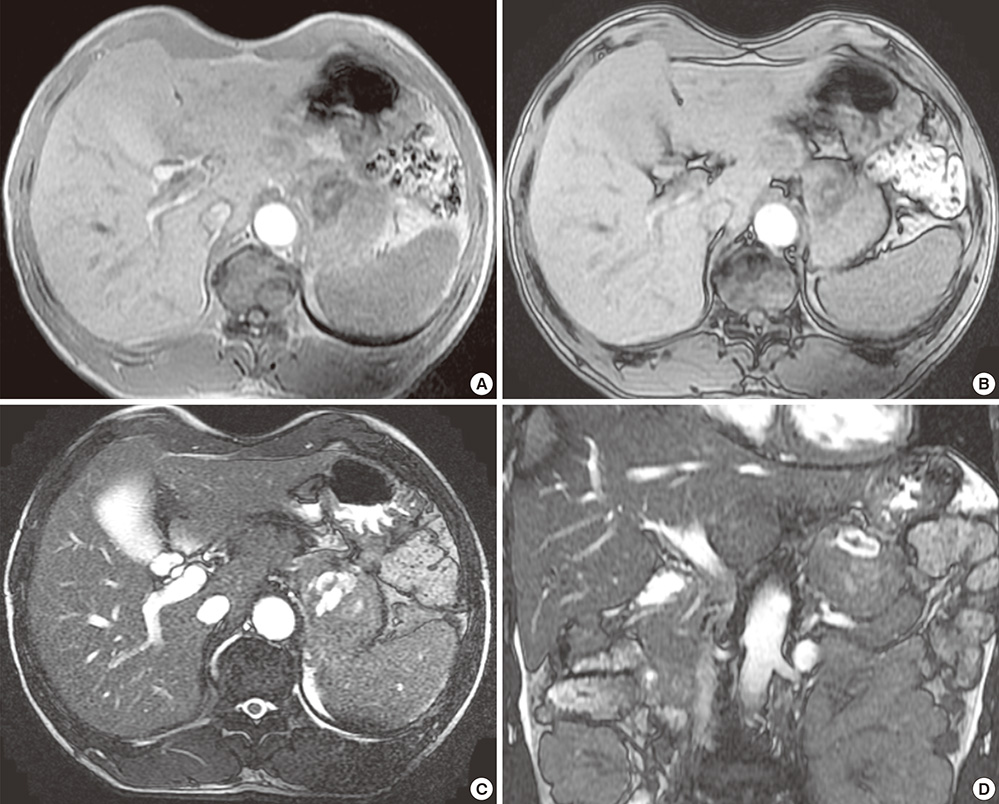
Fig. 3 Adrenocortical oncocytoma in a 54-yr-old man (Case 2), MR images. The mass primarily demonstrates hypointensity on in-phase T1WI MR imaging (A) without a definite signal drop on the opposed-phase T1WI MR imaging (B), with a central hemorrhagic necrotic component. On T2WI MR imaging (C, axial; D, coronal), this mass is primarily of slightly high signal intensity with a central hyperintense portion.
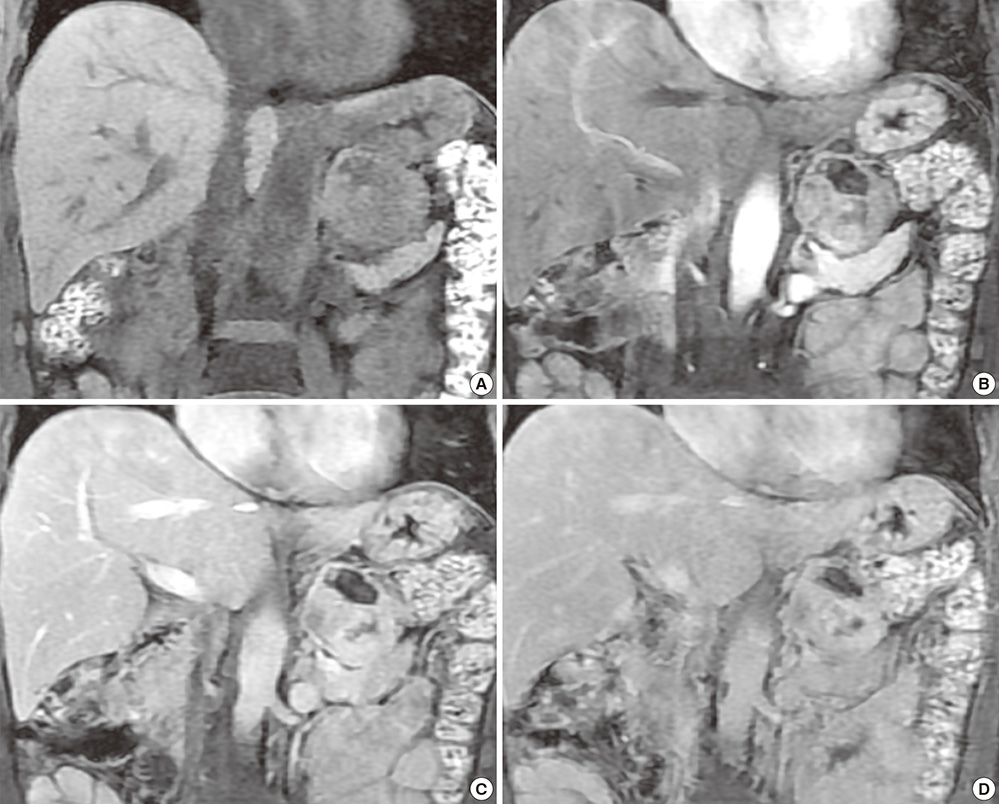
Fig. 4 Adrenocortical oncocytoma in a 54-yr-old man (Case 2), contrast-enhanced MR images. (A) Precontrast (B-D) Thoroughly heterogeneous enhancement of a solid tumoral portion at the 1-min (B), peak enhancement at 3-min (C), and slight enhancement washout at the 5-min delayed phases (D). Intratumoral hemorrhagic necrosis is visualized as a constantly non-enhancing portion.
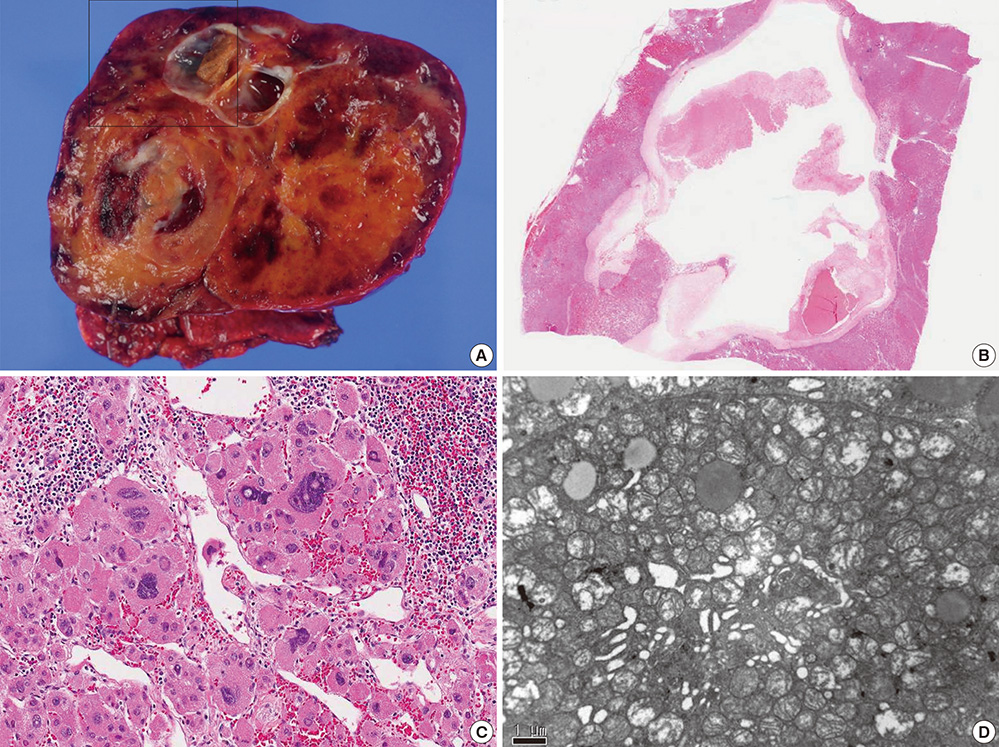
Fig. 5 Adrenocortical oncocytoma in a 54-yr-old man (Case 2), gross and microscopic findings. (A, B) The tumor was an oval-shaped soft mass that was encapsulated by a thin fibrous capsule and a multifocal brownish hemorrhage with a focal cystic change. (C) The tumor was composed of epithelial cells with abundant acidophilic cytoplasm, nuclear pleomorphism, and a diffuse growth pattern, as observed using a light microscope. (D) By electron microscopy, the oncocytic cytoplasm was filled with a large number of mitochondria, as well as some lysosomes, Golgi bodies, small lipid particles, and glycogen particles.
Reference
-
1. Nguyen GK, Vriend R, Ronaghan D, Lakey WH. Heterotopic adrenocortical oncocytoma: a case report with light and electron microscopic studies. Cancer. 1992; 70:2681–2684.2. Kakimoto S, Yushita Y, Sanefuji T, Kondo A, Fujishima N, Kishikawa M, Matsumoto K. Non-hormonal adrenocortical adenoma with oncocytoma-like appearances. Hinyokika Kiyo. 1986; 32:757–763.3. Geramizadeh B, Norouzzadeh B, Bolandparvaz S, Sefidbakht S. Functioning adrenocortical oncocytoma: a case report and review of literature. Indian J Pathol Microbiol. 2008; 51:237–239.4. Akatsu T, Kameyama K, Araki K, Ashizawa T, Wakabayashi G, Kitajima M. Functioning adrenocortical oncocytoma: the first documented case producing interleukin-6 and review of the literature. J Endocrinol Invest. 2008; 31:68–73.5. Gołkowski F, Buziak-Bereza M, Huszno B, Bałdys-Waligórska A, Stefańska A, Budzyński A, Okoń K, Chrzan R, Urbanik A. The unique case of adrenocortical malignant and functioning oncocytic tumour. Exp Clin Endocrinol Diabetes. 2007; 115:401–404.6. Xiao GQ, Pertsemlidis DS, Unger PD. Functioning adrenocortical oncocytoma: a case report and review of the literature. Ann Diagn Pathol. 2005; 9:295–297.7. Erlandson RA, Reuter VE. Oncocytic adrenal cortical adenoma. Ultrastruct Pathol. 1991; 15:539–547.8. Wong DD, Spagnolo DV, Bisceglia M, Havlat M, McCallum D, Platten MA. Oncocytic adrenocortical neopla: a clinicopathologic study of 13 new cases emphasizing the importance of their recognition. Hum Pathol. 2011; 42:489–499.9. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol. 1998; 170:747–752.10. Bisceglia M, Ludovico O, Di Mattia A, Ben-Dor D, Sandbank J, Pasquinelli G, Lau SK, Weiss LM. Adrenocortical oncocytic tumors: report of 10 cases and review of the literature. Int J Surg Pathol. 2004; 12:231–243.11. El-Naggar AK, Evans DB, Mackay B. Oncocytic adrenal cortical carcinoma. Ultrastruct Pathol. 1991; 15:549–556.12. Kitching PA, Patel V, Harach HR. Adrenocortical oncocytoma. J Clin Pathol. 1999; 52:151–153.13. Defossez SM, Yoder IC, Papanicolaou N, Rosen BR, McGovern F. Nonspecific magnetic resonance appearance of renal oncocytomas: report of 3 cases and review of the literature. J Urol. 1991; 145:552–554.14. Kim JI, Cho JY, Moon KC, Lee HJ, Kim SH. Segmental enhancement inversion at biphasic multidetector CT: characteristic finding of small renal oncocytoma. Radiology. 2009; 252:441–448.15. Shah RK, Oto A, Ozkan OS, Ernst RD, Hernandez JA, Chaudhary HB, Koroglu M. Adrenal oncocytoma: US and CT findings. JBR-BTR. 2004; 87:180–182.16. Mitchell DG, Crovello M, Matteucci T, Petersen RO, Miettinen MM. Benign adrenocortical masses: diagnosis with chemical shift MR imaging. Radiology. 1992; 185:345–351.17. McLoughlin RF, Bilbey JH. Tumors of the adrenal gland: findings on CT and MR imaging. AJR Am J Roentgenol. 1994; 163:1413–1418.18. Gandras EJ, Schwartz LH, Panicek DM, Levi G. Case report: adrenocortical oncocytoma: CT and MRI findings. J Comput Assist Tomogr. 1996; 20:407–409.
