Pulmonary Bone Cement Embolism: CT Angiographic Evaluation with Material Decomposition Using Gemstone Spectral Imaging
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Hospital Bucheon, Bucheon 420-767, Korea. acarad@naver.com
- KMID: 1731047
- DOI: http://doi.org/10.3348/kjr.2014.15.4.443
Abstract
- We report a case of pulmonary bone cement embolism in a female who presented with dyspnea following multiple sessions of vertebroplasty. She underwent spectral CT pulmonary angiography and the diagnosis was made based on enhanced visualization of radiopaque cement material in the pulmonary arteries and a corresponding decrease in the parenchymal iodine content. Here, we describe the CT angiography findings of bone cement embolism with special emphasis on the potential benefits of spectral imaging, providing additional information on the material composition.
MeSH Terms
Figure
-
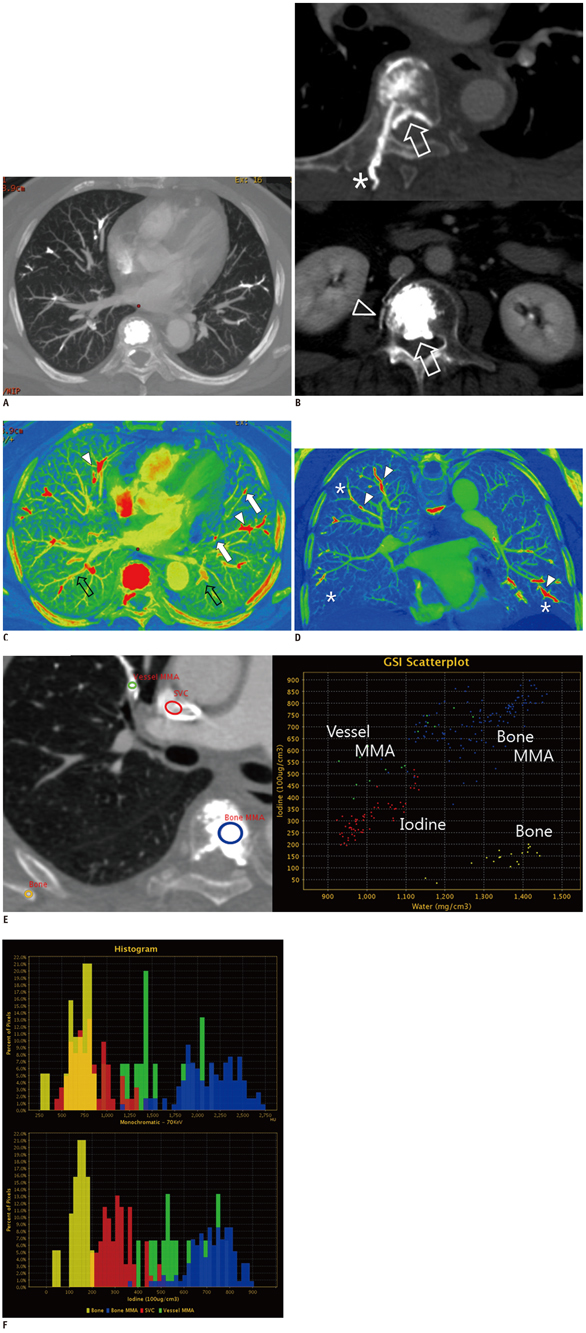
Fig. 1 Spectral CT angiography of 56-year-old woman admitted for intermittent dyspnea and hypotension. A. Axial maximal-intensity projection (MIP) image from monochromatic reconstruction at 140 kVp revealed bone cement emboli of variable sizes and shapes in lobar, segmental, and subsegmental pulmonary arteries of right middle and both lower lobes. This MIP image was reconstructed at 10-mm thickness. B. Multiplanar reconstruction images showed multifocal epidural cement leakage in epidural spaces at thoracic and lumbar vertebral levels (arrows). Bone cement extended to back muscle through needle tract (*) at sixth thoracic vertebral level (upper). Axial image at level of third lumbar vertebral body demonstrated origin of leak, showing cement in right laterovertebral vein (arrowhead). C. Axial iodine, material-density image (iodine map) created from gemstone spectral imaging (GSI) software at same level shown in Figure 1A demonstrated multiple pulmonary cement emboli in red (arrowheads) and corresponding decrease in parenchymal iodine content. Compared with Figure 1A, iodine map more clearly demonstrated smaller bone cement-emboli in segmental and subsegmental arteries (arrows). Note amorphous pink casts (open arrows) in multiple pulmonary arterial branches, shown to be dense iodinated blood, not cement materials, on GSI scatter plot (data not shown). D. Iodine map reconstructed in oblique coronal plane, passing from posterosuperior to anteroinferior, allowed direct visualization of embolic materials within pulmonary arteries (arrowheads). Corresponding underperfused area (*) correlated with embolic-occluded pulmonary arterial vascular territory. E. Gemstone spectral imaging (GSI) scatter plot for material separation showed similar compositions of pulmonary emboli and bone cement in vertebral body. However, it demonstrated that bone, bone cement, and iodinated contrast in this patient had different compositions although all of them show similar high attenuation in monochromatic image. Iodine, bone, and bone cement were represented on iodine (water) material density pairs using GSI scatter plot. F. Hounsfield unit (upper) and iodine content (lower) histograms of region of interest in Figure 1E. In this case, iodinated contrast had overlapping density with bone and cement emboli on Hounsfield unit based histogram created from 70 KeV monochromatic spectral energy (upper). However, in iodine content histogram (lower), these materials were clearly separated. Furthermore, positions of pulmonary embolus and vertebral bone cement showed considerable overlap, suggesting that these two materials had identical or similar compositions and that pulmonary embolus had originated from cement material in vertebral body.
Reference
-
1. Galibert P, Deramond H, Rosat P, Le Gars D. [Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty]. Neurochirurgie. 1987; 33:166–168.2. Krueger A, Bliemel C, Zettl R, Ruchholtz S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: a systematic review of the literature. Eur Spine J. 2009; 18:1257–1265.3. Barragán-Campos HM, Vallée JN, Lo D, Cormier E, Jean B, Rose M, et al. Percutaneous vertebroplasty for spinal metastases: complications. Radiology. 2006; 238:354–362.4. Choe DH, Marom EM, Ahrar K, Truong MT, Madewell JE. Pulmonary embolism of polymethyl methacrylate during percutaneous vertebroplasty and kyphoplasty. AJR Am J Roentgenol. 2004; 183:1097–1102.5. Remy-Jardin M, Pistolesi M, Goodman LR, Gefter WB, Gottschalk A, Mayo JR, et al. Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology. 2007; 245:315–329.6. Lu GM, Wu SY, Yeh BM, Zhang LJ. Dual-energy computed tomography in pulmonary embolism. Br J Radiol. 2010; 83:707–718.7. Lu GM, Zhao Y, Zhang LJ, Schoepf UJ. Dual-energy CT of the lung. AJR Am J Roentgenol. 2012; 199:5 Suppl. S40–S53.8. Sun YS, Zhang XY, Cui Y, Tang L, Li XT, Chen Y, et al. Spectral CT imaging as a new quantitative tool? Assessment of perfusion defects of pulmonary parenchyma in patients with lung cancer. Chin J Cancer Res. 2013; 25:722–728.9. Ghaye B. Peripheral pulmonary embolism on multidetector CT pulmonary angiography. JBR-BTR. 2007; 90:100–108.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Asymptomatic Bone Cement Pulmonary Embolism after Percutaneous Vertebroplasty: A Case Report
- Pulmonary Bone Cement Embolism Following Percutaneous Vertebroplasty
- Transcatheter Removal of Bone Cement Embolism in the Right Atrium after Percutaneous Vertebroplasty: The Embolus Broke in Half and Migrated to the Right Pulmonary Artery Intraoperatively
- Multidetector CT Findings of Polymethylmethacrylate Cement Leakage Inducing Inferior Vena Cava Thrombosis: A Case Report
- A Case of Fatal Pulmonary Embolism Caused by Bone Cement after Percutaneous Vertebroplasty
