Traumatic Cervical Cord Transection without Facet Dislocations-A Proposal of Combined Hyperflexion-Hyperextension Mechanism: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Korea University College of Medicine, Seoul, Korea. jcjks@unitel.co.kr
- KMID: 1714054
- DOI: http://doi.org/10.3346/jkms.2010.25.8.1247
Abstract
- A patient is presented with a cervical spinal cord transection which occurred after a motor vehicle accident in which the air bag deployed and the seat belt was not in use. The patient had complete quadriplegia below the C5 level and his imaging study showed cervical cord transection at the level of the C5/6 disc space with C5, C6 vertebral bodies and laminar fractures. He underwent a C5 laminectomy and a C4-7 posterior fusion with lateral mass screw fixation. Previous reports have described central cord syndromes occurring in hyperextension injuries, but in adults, acute spinal cord transections have only developed after fracture-dislocations of the spine. A case involving a post-traumatic spinal cord transection without any evidence of radiologic facet dislocations is reported. Also, we propose a combined hyperflexion-hyperextension mechanism to explain this type of injury.
Keyword
MeSH Terms
Figure
-

Fig. 1 C5 and C6 wedge compression fractures with minimal C5 retrolisthesis on C6 are revealed on a plain lateral cervical film, but there is no evidence of dislocation of the facet joints.
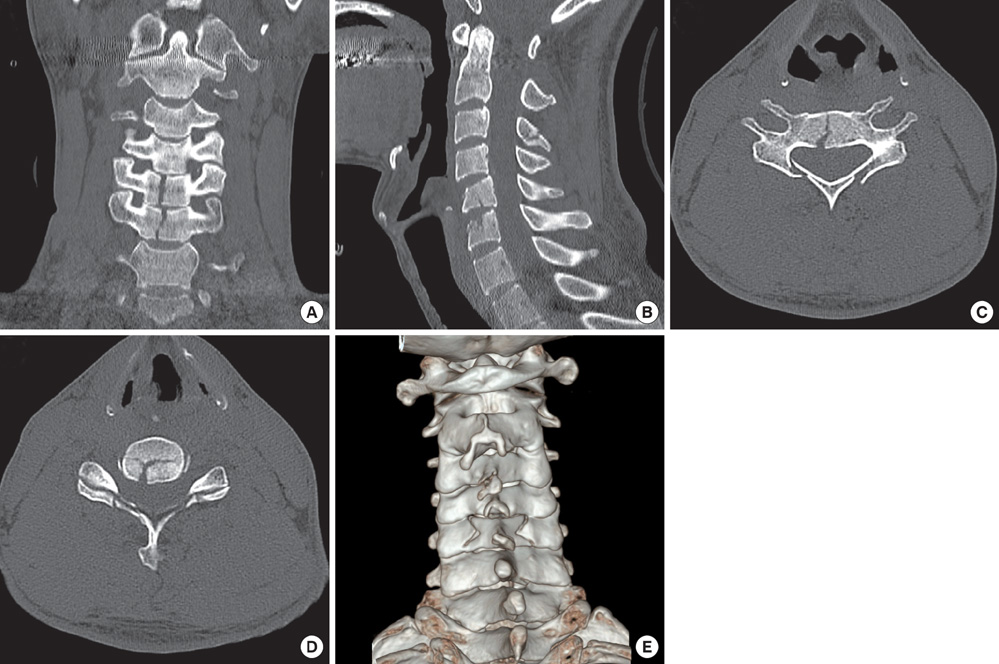
Fig. 2 Cervical spine computed tomographic (CT) scans with 3-dimensional (3-D) reconstruction. (A) C5 and C6 vertebral bodies show vertical fracture centrums in a coronally reconstructed image. (B) Only subtle C5 retrolisthesis on C6 is noted on a sagittally reconstructed image. A C3 spinous process fracture is also identified. (C) The axial section of the C5 vertebra at the pedicle level shows a depressed laminar fracture. (D) The fracture lines of the C5 lamina are through the lamina-facet junction. The C5/6 facet joints are intact. (E) 3-D reconstructed image shows a C5 lamina depressed fracture through the lamina-facet junction.

Fig. 3 T2-weighted magnetic resonance image reveals a horizontal line of high signal intensity in the cervical spinal cord at the C5/6 disc space level which represents spinal cord transection. Severe cord swelling around the injured level and edema of the C5, C6 vertebral bodies are also noted.
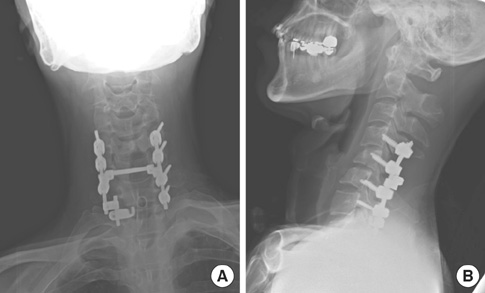
Fig. 4 Plain radiographic flims 4 months postoperatively. The right C7 lateral mass was cleaved during the screw insertion, so a lamina hook was used. (A) Anteriorposterior view. (B) Lateral view.
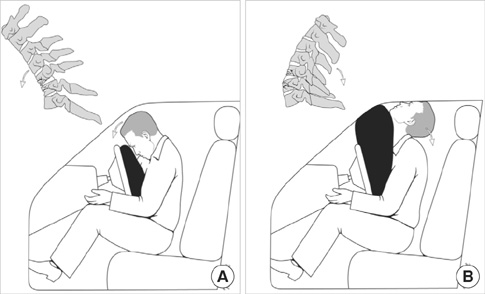
Fig. 5 Summarization of the hypothesized mechanism of the injury. (A) During the initial short moment of the collision, the airbag is just in contact with the torso, but not with the face of the patient. As a result, compressive flexion force interacts at the cervical spine, resulting in C5, C6 vertebral body fractures. (B) In the late stage, the patient override the airbag, which causes him to hit his head on the roof and windshield of the vehicle, resulting in acute cervical hyperextension. The spinal cord transection occurs by posterior displacement of the C5 vertebral body against the cord in this powerful distractive extension injury.
Reference
-
1. Kalfas I, Wilberger J, Goldberg A, Prostko ER. Magnetic resonance imaging in acute spinal cord trauma. Neurosurgery. 1988. 23:295–299.
Article2. Crenshaw AH Jr, Wood GW 2nd, Wood MW Jr, Ray MW. Fracture and dislocation of the fourth and fifth cervical vertebral bodies with transection of the spinal cord. Clin Orthop Relat Res. 1989. 248:158–162.
Article3. Deeb ZL, Rothfus WE, Goldberg AL, Daffner RH. Absent cord sign in acute spinal trauma. Clin Imaging. 1990. 14:138–142.
Article4. Fasano FJ Jr, Stauffer ES. Traumatic division of the spinal cord demonstrated by magnetic resonance imaging. Report of two cases. Clin Orthop Relat Res. 1988. 233:168–170.5. Mendelsohn DB, Zollars L, Weatherall PT, Girson M. MR of cord transection. J Comput Assist Tomogr. 1990. 14:909–911.6. Chieregato A. High cervical spinal cord complete transection. Arch Neurol. 2008. 65:1126.
Article7. Aarabi B, Koltz M, Ibrahimi D. Hyperextension cervical spine injuries and traumatic central cord syndrome. Neurosurg Focus. 2008. 25:E9.
Article8. Bicknell JM, Fielder K. Unrecognized incomplete cervical spinal cord injury: review of nine new and 28 previously reported cases. Am J Emerg Med. 1992. 10:336–343.
Article9. Epstein N, Epstein JA, Benjamin V, Ransohoff J. Traumatic myelopathy in patients with cervical spinal stenosis without fracture or dislocation: methods of diagnosis, management, and prognosis. Spine (Phila Pa 1976). 1980. 5:489–496.
Article10. Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg. 1954. 11:546–577.11. Berlot G, Viviani M, Gullo A, Magnaldi S. Delayed traumatic cervical cord transection. Am J Emerg Med. 1995. 13:101–103.
Article12. Crandall JR, Kuhlmann TP, Pilkey WD. Air and knee bolster restraint system: laboratory sled tests with human cadavers and the Hybrid III dummy. J Trauma. 1995. 38:517–520.13. Pang D, Pollack IF. Spinal cord injury without radiographic abnormality in children--the SCIWORA syndrome. J Trauma. 1989. 29:654–664.
Article14. Taylor AR. The mechanism of injury to the spinal cord in the neck without damage to vertebral column. J Bone Joint Surg Br. 1951. 33-B:543–547.15. Allen BL Jr, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1982. 7:1–27.
Article16. Dvorak MF, Fisher CG, Fehlings MG, Rampersaud YR, Oner FC, Aarabi B, Vaccaro AR. The surgical approach to subaxial cervical spine injuries: an evidence-based algorithm based on the SLIC classification system. Spine (Phila Pa 1976). 2007. 32:2620–2629.17. Lim PA, Tow AM. Recovery and regeneration after spinal cord injury: a review and summary of recent literature. Ann Acad Med Singapore. 2007. 36(1):49–57.18. Kirshblum S, Millis S, McKinley W, Tulsky D. Late neurologic recovery after traumatic spinal cord injury. Arch Phys Med Rehabil. 2004. 85:1811–1817.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Cervical Spine Injuries without Fracture or Dislocation
- The cervical spinal fractures : comparison of the sites and incidences according to the causes and the types of the injuries
- Unilateral Facet dislocation of Lumbosacral Junction: a case report
- Non-Contiguous Spinal Injury in Cervical Spinal Trauma: Evaluation with Cervical Spine MRI
- MR Imaging of Cord Transection without Skeletal Injury: A case Report
