Monoblock Craniofacial Internal Distraction in a Child with Pfeiffer Syndrome: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Ajou University School of Medicine, Suwon, Korea. ee80@unitel.co.kr
- 2Department of Plastic and Reconstructive Surgery, Ajou University School of Medicine, Suwon, Korea.
- KMID: 1713473
- DOI: http://doi.org/10.3346/jkms.2008.23.2.342
Abstract
- A 7-yr-old boy visited our surgical center with Pfeiffer syndrome type 1, presenting with macrocrania, broad big toe and thumb, exophthalmos, tongue protrusion, malocclusion with midfacial retrusion, mild respiratory difficulty due to minor upper airway obstruction, and developmental delay. He also exhibited anthrophobia with a passive character. The patient was treated with internal monoblock distraction osteogenesis to increase the intracranial and intraorbital volumes, and the nasal and pharyngeal airway spaces using two modular mid-facial internal distractors. For distraction, the latency period was 1 week, the daily activation of 1.0 mm was 20 days (total advancement 20 mm at the midline), and the consolidation period was 3 months. The follow-up computed tomography 12 months after surgery showed expansion of the brain and proper ossification in the distracted area. The patient also showed aesthetically good cranial contours, improved tongue and eyeball protrusion, no respiratory difficulty, and improved learning. We suggest that the internal distraction may last longer than an external type, resulting in a better bone fusion rate and successful expansion of craniofacial bones.
MeSH Terms
Figure
-

Fig. 1 Upper: preoperative three-dimensional reconstruction images of computed tomography show bulging skull of the anterior fontanelle (red arrows), underdevelopment of frontal bone (yellow arrows), small face, and malocclusion with midfacial retrusion (white arrows). Lower: preoperative photos show exophthalmos (yellow arrows), malocclusion and tongue protrusion (white arrow) due to midfacial retrusion.
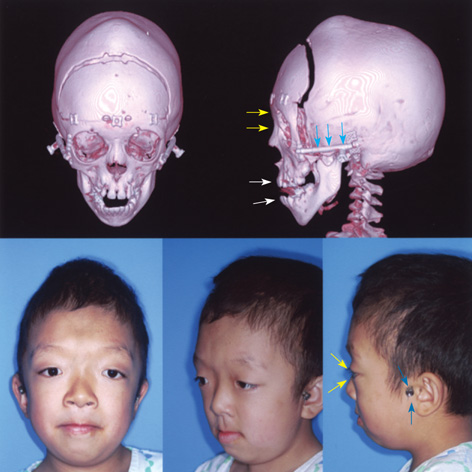
Fig. 2 Upper: postoperative three-dimensional reconstruction images of computed tomography at 2 months after surgery show forward advancement of fronto-facial monoblock (yellow arrows) and improved malocclusion (white arrows) with a distraction rod (blue arrows). Lower: postoperative photos show improved exophthalmos (yellow arrows) and malocclusion, disappearance of tongue protrusion after midfacial advancement with a distraction rod (blue arrows) exposed on the temporal scalp.
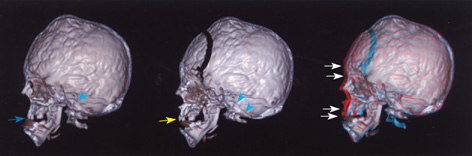
Fig. 3 Conceptual illustration of the preoperative, postoperative and overlapped images of the cranio-facial bony contour in the three-dimensional computed tomography. Left: preoperative image shows small face, malocclusion with midfacial retrusion (blue arrow), and slanted clival angle (blue arrow heads). Middle: postoperative image shows improved malocclusion (yellow arrow) and slanted clival angle (blue arrow heads). Right: the overlapping image based on the clival angle shows forward advancement (white arrows) of cranio-facial monoblock bone flap (red color), compared with preoperative craniofacial contour (blue color).

Fig. 4 One year follow-up computed tomography images of three-dimensional reconstruction show bony fusion in the cranial advancement area (white arrows) and in the maxillary bone (green arrows) with improved occlusion of teeth (red arrows). Lower: one-year follow-up photos show nearly normal facial contours.
Cited by 1 articles
-
Pfeiffer Syndrome Type 2 with Sporadic Fibroblast Growth Factor Receptor 2 Mutation and Coccygeal Anomaly
Jin Sun Lee, Jin Hyuk Choi, Yong Wook Lee, Mi Hyeon Gang, Sun Kyoung You, Hyun Dea Shin, Mea-young Chang
Perinatology. 2018;29(3):128-132. doi: 10.14734/PN.2018.29.3.128.
Reference
-
1. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992. 89:1–8.
Article2. Polley JW, Figueroa AA, Charbel FT, Berkowitz R, Reisberg D, Cohen M. Monobloc craniomaxillofacial distraction osteogenesis in a newborn with severe craniofacial synostosis: a preliminary report. J Craniofac Surg. 1995. 6:421–423.3. Polley JW, Figueroa AA. Management of severe maxillary deficiency in childhood and adolescence through distraction osteogenesis with an external, adjustable, rigid distraction device. J Craniofac Surg. 1997. 8:181–185.
Article4. Fearon JA. Halo distraction of the Le Fort III in syndromic craniosynostosis: a long-term assessment. Plast Reconstr Surg. 2005. 115:1524–1536.
Article5. Riediger D, Poukens JM. Le Fort III osteotomy: a new internal positioned distractor. J Oral Maxillofac Surg. 2003. 61:882–889.
Article6. Cohen SR, Rutrick RE, Burstein FD. Distraction osteogenesis of the human craniofacial skeleton: initial experience with new distraction system. J Craniofac Surg. 1995. 6:368.7. Chin M, Toth BA. Le Fort III advancement with gradual distraction using internal devices. Plast Reconstr Surg. 1997. 100:819–830.
Article8. Cohen SR, Holmes RE. Internal Le Fort III distraction with biodegradable devices. J Craniofac Surg. 2001. 12:264–272.
Article9. Gosain AK. Plastic Surgery Educational Foundation DATA Committee. Distraction osteogenesis of the craniofacial skeleton. Plast Reconstr Surg. 2001. 107:278–280.
Article10. Lee YK, Choi JH, Kim SH, Baek SH, Chang YI. Midfacial distraction osteogenesis of Crouzon syndrome with RED (Rigid External Distraction) system. Korean J Orthod. 2002. 32:175–183.11. Tessier P. The definitive plastic surgical treatment of the severe facial deformities of craniofacial dysostosis: Crouzon's and Apert's diseases. Plast Reconstr Surg. 1971. 48:419–442.
Article12. Ortiz-Monasterio F, del Campo AF, Carrillo A. Advancements of the orbits and the midface in one piece, combined with frontal repositioning, for the correction of Crouzon's deformities. Plast Reconstr Surg. 1978. 61:507–516.13. McCarthy JG, Glasberg SB, Cutting CB, Epstein FJ, Grayson BH, Ruff G, Thorne CH, Wisoff J, Zide BM. Twenty-year experience with early surgery for craniosynostosis. II. The craniofacial synostosis syndromes and pansynostosis-Results and unsolved problems. Plast Reconstr Surg. 1995. 96:284–295.14. Hirabayashi S, Sugawara Y, Sakurai A, Harii K, Park S. Frontoorbital advancement by gradual distraction. Technical note. J Neurosurg. 1998. 89:1058–1061.15. Uemura T, Hayashi T, Satoh K, Mitsukawa N, Yoshikawa A, Jinnnai T, Hosaka Y. A case of improved obstructive sleep apnea by distraction osteogenesis for midface hypoplasia of an infantile Crouzon's syndrome. J Craniofac Surg. 2001. 12:73–77.
Article16. Iannetti G, Fadda T, Agrillo A, Poladas G, Iannetti G, Filiaci F. LeFort III advancement with and without osteogenesis distraction. J Craniofac Surg. 2006. 17:536–543.
Article17. Mitsukawa N, Satoh K, Hayashi T, Furukawa Y, Uemura T, Hosaka Y. A reflectable case of obstructive sleep apnea in an infant with Crouzon syndrome. J Craniofac Surg. 2004. 15:874–878.
Article18. Fearon JA, Whitaker LA. Complications with facial advancement:a comparison between the Le Fort III and monobloc advancements. Plast Reconstr Surg. 1993. 91:990–995.19. Kubler AC, Speder B, Zoller JE. Fronto-orbital advancement with simultaneous LeFort III-distraction. J Craniomaxillofac Surg. 2004. 32:291–295.20. Gosain AK, Santoro TD, Havlik RJ, Cohen SR, Holmes RE. Midface distraction following Le Fort III and monobloc osteotomies: problems and solutions. Plast Reconstr Surg. 2002. 109:1797–1808.
Article21. Akizuki T, Komuro Y, Ohmori K. Distraction osteogenesis for craniosynostosis. Neurosurg Focus. 2000. 9(3):e1.
Article22. Chung J, Yoon SH. Rotating distraction osteogenesis in a child with secondary craniosyntostosis. J Craniofac Surg. 2006. 17:557–560.
Article23. Anderson PJ, Tan E, David DJ. Simultaneous multiple vector distraction for craniosynostosis syndromes. Br J Plast Surg. 2005. 58:626–631.
Article24. Holmes AD, Wright GW, Meara JG, Heggie AA, Probert TC. LeFort III internal distraction in syndromic craniosynostosis. J Craniofac Surg. 2002. 13:262–272.
Article25. Nishimoto S, Oyama T, Nagashima T, Shimizu F, Tsugawa T, Takeda M, Toda N. Gradual distraction fronto-orbital advancement with 'floating forehead' for patients with syndromic craniosynostosis. J Craniofac Surg. 2006. 17:497–505.
Article26. Wiltfang J, Hirschfelder U, Neukam FW, Kessler P. Long-term results of distraction osteogenesis of the maxilla and midface. Br J Oral Maxillofac Surg. 2002. 40:473–479.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pfeiffer Syndrome
- A Case Report of Pfeiffer Syndrome with Spinal Anomaly
- Midfacial distraction osteogenesis of Crouzon syndrome with RED(Rigid External Distraction) system
- A case of Pfeiffer syndrome with c833_834GC>TG (Cys278Leu) mutation in the FGFR2 gene
- Distraction Osteogenesis Of The Midface With A Rigid External Distractor (RED)
