J Korean Med Sci.
2008 Apr;23(2):320-323. 10.3346/jkms.2008.23.2.320.
Complete Hematopoietic Recovery after Continuous Iron Chelation Therapy in a Patient with Severe Aplastic Anemia with Secondary Hemochromatosis
- Affiliations
-
- 1Division of Hematology and Oncology, Our Lady of Mercy Hospital, The Catholic University of Korea, Incheon, Korea. hellenpark@hanmail.net
- KMID: 1713468
- DOI: http://doi.org/10.3346/jkms.2008.23.2.320
Abstract
- A 16-yr-old male patient with hemochromatosis due to multiple packed red blood cell transfusions was referred to our emergency center for the treatment of severe aplastic anemia and dyspnea. He was diagnosed with aplastic anemia at 11-yr of age. He had received continuous transfusions because an HLA-matched marrow donor was unavailable. Following a continuous, approximately 5-yr transfusion, he was noted to develop hemochromatosis. He had a dilated cardiomyopathy and required diuretics and digitalis, multiple endocrine and liver dysfunction, generalized bleeding, and skin pigmentation. A total volume of red blood cell transfusion before deferoxamine therapy was about 96,000 mL. He received a regular iron chelation therapy (continuous intravenous infusion of deferoxamine, 50 mg/kg/day for 5 days q 3-4 weeks) for approximately seven years after the onset of multiple organ failures. His cytopenia and organ dysfunctions began to be gradually recovered since about 2002, following a 4-yr deferoxamine treatment. He showed completely normal ranges of peripheral blood cell counts, heart size, and liver function two years ago. He has not received any transfusions for the last four years. This finding suggests that a continuous deferoxamine infusion may play a role in the immune regulation in addition to iron chelation effect.
Keyword
MeSH Terms
Figure
-
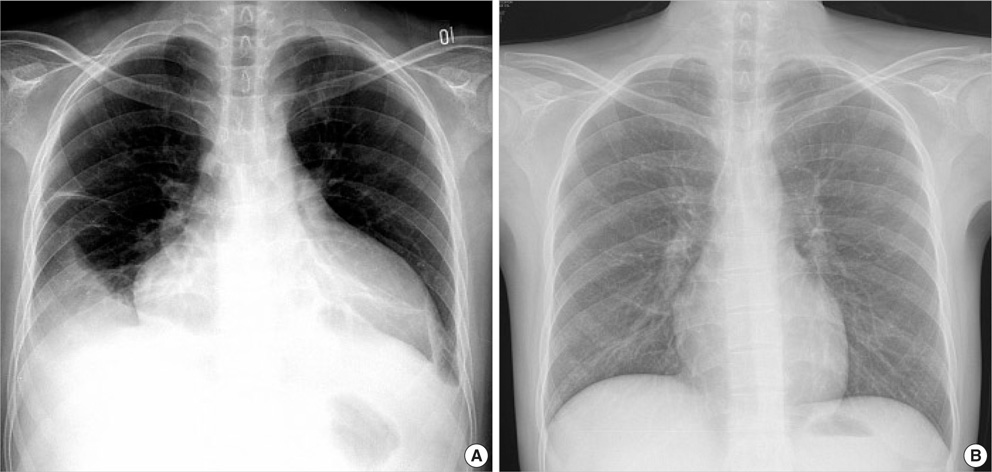
Fig. 1 Posteroanterior chest radiographs reveal a marked cardiomegaly with right pleural effusion before the treatment (A) and a normalized heart after the deferoxamine therapy (B).

Fig. 2 Hemoglobin changes before and after deferoxamine therapy.
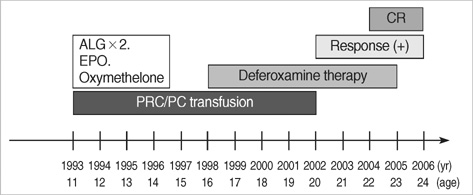
Fig. 3 The full clinical course of the patient: Pre- and post-deferoxamine therapy. ALG, anti-lymphocyte globulin; EPO, erythropoietin; PRC, packed red blood cell; PC, platelet concentrate; CR, complete response.
Reference
-
1. Keohane EM. Acquired aplastic anemia. Clin Lab Sci. 2004. 17:165–171.2. Geissler K. Pathophysiology and treatment of aplastic anemia. Wien Klin Wochenschr. 2003. 115:444–450.
Article3. Maciejewski JP, Risitano AM. Aplastic anemia: management of adult patients. Hematolgoy Am Soc Hematol Educ Program. 2005. 110–117.
Article4. Mwanda OW, Otieno CF, Abdalla FK. Transfusion haemosiderosis inspite of regular use of desferrioxamine: case report. East Afr Med J. 2004. 81:326–328.
Article5. Girot R, Thévenin M, Bouveret JP, Jeannel F, Rymer JC. Treatment of iron overload due to repeated transfusions with subcutaneous infusions of desferrioxamine. Arch Fr Pediatr. 1980. 37:241–247.6. Cohen AR, Mizanin J, Schwartz E. Rapid removal of excessive iron with daily, high-dose intravenous chelation therapy. J Pediatr. 1989. 115:151–155.
Article7. Lee JH, Lee JH, Shin YR, Lee JS, Kim WK, Chi HS, Park CJ, Lee KH. Spontaneous remission of aplastic anemia: a retrospective analysis. Haematologica. 2001. 86:928–933.8. Carotenuto P, Pontesilli O, Cambier JC, Hayward AR. Desferoxamine blocks IL 2 receptor expression on human T lymphocytes. J Immunol. 1986. 136:2342–2347.9. Hoffbrand AV, Ganeshaguru K, Hooton JW, Tattersall MH. Effect of iron deficiency and desferrioxamine on DNA synthesis in human cells. Br J Haematol. 1976. 33:517–526.
Article10. Shao Z, Chu Y, Zhang Y, Chen G, Zheng Y. Treatment of severe aplastic anemia with an immunosuppressive agent plus recombinant human granulocyte-macrophage colony-stimulating factor and erythropoietin. Am J Hematol. 1998. 59:185–191.
Article11. Bessho M, Hirashima K, Asano S, Ikeda Y, Ogawa N, Tomonaga M, Toyama K, Nakahata T, Nomura T, Mizoguchi H, Yoshida Y, Niitsu Y, Kohgo Y; Multicenter Study Group. Treatment of the anemia of aplastic anemia patients with recombinant human erythropoietin in combination with granulocyte colony-stimulating factor: a multicenter randomized controlled study. Eur J Haematol. 1997. 58:265–272.12. Aucella F, Vigilante M, Scalzulli P, Musto P, Prencipe M, Valente GL, Carotenuto M, Stallone C. Synergistic effect of desferrioxamine and recombinant erythropoietin on erythroid precursor proliferation in chronic renal failure. Nephrol Dial Transplant. 1999. 14:1171–1175.
Article13. Kling PJ, Dragsten PR, Roberts RA, Dos Santos B, Brooks DJ, Hedlund BE, Taetle R. Iron deprivation increases erythropoietin production in vitro, in normal subjects and patients with malignancy. Br J Haematol. 1996. 95:241–248.14. Tsironi M, Deftereos S, Andriopoulos P, Farmakis D, Meletis J, Aessopos A. Reversal of heart failure in thalassemia major by combined chelation therapy: a case report. Eur J Haematol. 2005. 74:84–85.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and treatment of transfusion-related iron overload
- Diabetes mellitus caused by secondary hemochromatosis after multiple blood transfusions in 2 patients with severe aplastic anemia
- Secondary Hemochromatosis in a Patient with Aplastic Anemia: An autopsy case report
- A Case of Secondary Hemochromatosis Revealed in Gastrofiberscopy
- Acute Tubulointerstitial Nephritis Induced by Deferasirox following Hematopoietic Stem Cell Transplantation for Severe Aplastic Anemia
