Macrophage Activation Syndrome in Juvenile Rheumatoid Arthritis Successfully Treated with Cyclosporine A: A Case Report
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Department of Internal Medicine, Konkuk University Hospital, Konkuk University, 1 Hwayang-dong, Gwangjin-gu, Seoul, Korea. shlee@kuh.ac.kr
- KMID: 1713133
- DOI: http://doi.org/10.3346/jkms.2006.21.6.1124
Abstract
- Macrophage activation syndrome (MAS) is one of the serious complications of juvenile rheumatoid arthritis (JRA) and recently, cyclosporine A has been found to be effective in patients with corticosteroid-resistant MAS. A 29-yr-old male was admitted with high fever and jaundice for one month. He was diagnosed as juvenile arthritis 16 yr ago. Physical and laboratory results showed hepatosplenomegaly, high fever, pancytopenia and impaired liver and renal function tests, elevated triglyceride and serum ferritin levels. Bone marrow biopsy showed hyperplasia of histiocytes with active hemophagocytosis. He was diagnosed as MAS associated with juvenile rheumatoid arthritis and managed with high-dose corticosteroids initially, but clinical symptoms and laboratory findings did not improve immediately. Finally, he completely recovered after treatment with cyclosporine A (3 mg/kg/day).
MeSH Terms
Figure
-

Fig. 1 Radiographic images of hands, feet and hips. (A) Anteroposterior view of both hands shows that periarticular osteopenia and erosions at proximal interphalangeal, metacarpophalangeal, radiocarpal and radioulnar joints. Ankylosis at both carpometacarpal and intercarpal joints. (B) Anteroposterior view of both feet shows the periarticular erosions at metatarsotarsal, tibiotalar, talonavicular and naviculocuneiform joints. (C) Anteroposterior view of both hips shows that extensive pressure erosions in acetabuli and femoral heads, resulting in protrusion of the acetabuli, especially in right hip joint.
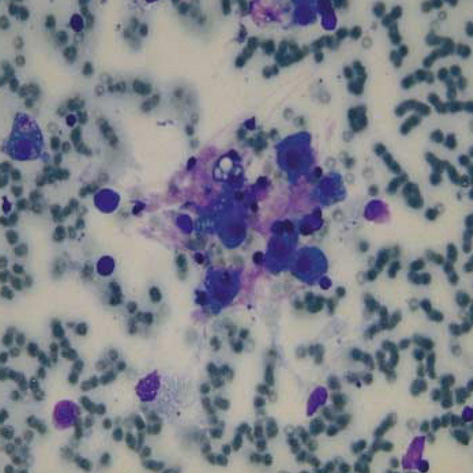
Fig. 2 Bone marrow aspiration. Cytopathology of bone marrow aspirates shows that histiocytes are markedly increased in number and some of them have active hemophagocytosis (Wright-Giemsa stain, ×400).
Reference
-
1. Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002. 14:548–552.
Article2. Grom AA, Passo M. Macrophage activation syndrome in systemic juvenile rheumatoid arthritis. J Pediatr. 1996. 129:630–632.3. Brewer EJ Jr, Bass J, Baum J, Cassidy JT, Firk C, Jacobs J, Harson V, Levirson JE, Schaller J, Stillman JS. Current proposed revision of JRA Criteria. JRA Criteria Subcommittee of the Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Section of the Arthritis Foundation. Arthritis Rheum. 1977. 20:Suppl. 195–199.4. Hadchouel M, Prieur AM, Griscelli C. Acute hemorrhagic, hepatic, and neurologic manifestations in juvenile rheumatoid arthritis: possible relationship to drugs or infection. J Pediatr. 1985. 106:561–566.
Article5. Stephan JL, Zeller J, Hubert P, Herbelin C, Dayer JM, Prieur AM. Macrophage activation syndrome and rheumatic disease in childhood: a report of four new cases. Clin Exp Rheumatol. 1993. 11:451–456.6. Athreya BH. Is macrophage activation syndrome a new entity? Clin Exp Rheumatol. 2002. 20:121–123.7. Ravelli A, Magni-Manzoni S, Foti T, Besana C, Felici E, Trail L, Garay S, Sala E, Pistorio A, Pavia AM. Macrophage activation syndrome in juvenile idiopathic arthritis: towards the development of diagnostic guidelines. Arthritis Rheum. 2001. 44:Suppl. 166.8. Henter JI. Biology and treatment of familial hemophagocytic lymphohistiocytosis: importance of perforin in lymphocyte-mediated cytotoxicity and triggering of apoptosis. Med Pediatr Oncol. 2002. 38:305–309.
Article9. Henter JI, Elinder G, Soder O, Hansson M, Andersson B, Andersson U. Hypercytokinemia in familial hemophagocytic lymphohistiocytosis. Blood. 1991. 78:2918–2922.
Article10. Stepp SE, Dufourcq-Lagelouse R, Le Deist F, Bhawan S, Certain S, Mathew PA, Henter JI, Bennett M, Fischer A, de Saint Basile G, Kumar V. Perforin gene defects in familial hemophagocytic lymphohistiocytosis. Science. 1999. 286:1957–1959.
Article11. Mouy R, Stephan JL, Pillet P, Haddad E, Hubert P, Prieur AM. Efficacy of cyclosporine A in the treatment of macrophage activation syndrome in juvenile arthritis: report of five cases. J Pediatr. 1996. 129:750–754.
Article12. Ravelli A, De Benedetti F, Viola S, Martini A. Macrophage activation syndrome in systemic juvenile rheumatoid arthritis successfully treated with cyclosporine. J Pediatr. 1996. 128:275–278.
Article13. Attur MG, Patel R, Thakker G, Vyas P, Levartovsky D, Patel P, Naqvi S, Raza R, Patel K, Abramson D, Bruno G, Abramson SB, Amin AR. Differential anti-inflammatory effects of immunosuppressive drugs: cyclosporin, rapamycin and FK-506 on inducible nitric oxide synthase, nitric oxide, cyclooxygenase-2 and PGE2 production. Inflamm Res. 2000. 49:20–26.
Article14. Lee JI, Ganster RW, Geller DA, Burckart GJ, Thomson AW, Lu L. Cyclosporine A inhibits the expression of costimulatory molecules on in vitro-generated dendritic cells: association with reduced nuclear translocation of nuclear factor kappa B. Transplantation. 1999. 68:1255–1263.15. Prahalad S, Bove KE, Dickens D, Lovell DJ, Grom AA. Etanercept in the treatment of macrophage activation syndrome. J Rheumatol. 2001. 28:2120–2124.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Macropharge Activation Syndrome Successfully Treated with Combination Therapy Including Etanercept
- Clinical significance of rheumatoid factor in juvenile rheumatoid arthritis
- Macrophage Activation Syndrome in a Child with Systemic Juvenile Rheumatoid Arthritis
- A case of fat embolism syndrome in juvenile rheumatoid arthritis patient
- Clinical observation on juvenile theumatoid arthritis
