Single Transconjunctival Incision and Two-point Fixation for the Treatment of Noncomminuted Zygomatic Complex Fracture
- Affiliations
-
- 1Department of Plastic Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea. pklee@catholic.ac.kr
- KMID: 1713123
- DOI: http://doi.org/10.3346/jkms.2006.21.6.1080
Abstract
- The ultimate goal in treating zygomatic complex fracture is to obtain an accurate, stable reduction while minimizing external scars and functional deformity. The present authors present our experiences with a single transconjunctival incision and two-point (inferior orbital rim and frontozygomatic suture) fixation in 53 patients with zygomatic complex fracture which were not comminuted. All patients had transconjunctival approaches with lateral canthal extensions, and six out of 53 patients also had an additional small (about less than 2 cm) gingivobuccal incision to achieve an accurate reduction. There were 3 minor complications, and the overall esthetics and functional results were satisfactory with a long term follow-up. Our method has the following advantages in the reduction of zygomatic complex fracture; It leaves only an inconspicuous lateral canthal scar. In addition, it provides excellent simultaneous visualization of the inferior orbital rim and frontozygomatic suture area. Hence, twopoint fixation through a single incision can be performed with a satisfactory stability.
MeSH Terms
Figure
-
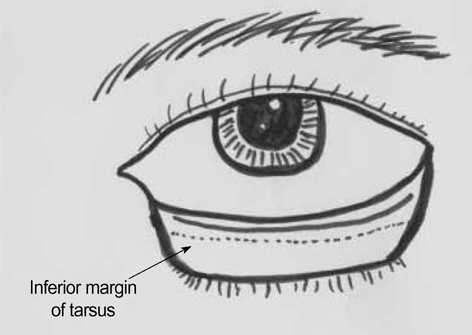
Fig. 1 After lateral canthal incision is made down to the periosteum of lateral orbital rim, the conjunctiva is incised 2, 3 mm below the tarsus from a point just lateral to the punctum to the lateral canthal incision site.
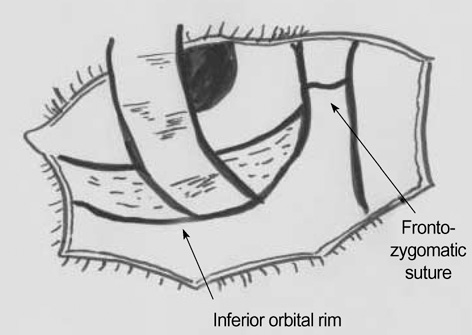
Fig. 2 By pulling the lower eyelid flap down and pulling the upper eyelid flap up, the entire lateral and inferior orbital rim can be exposed.
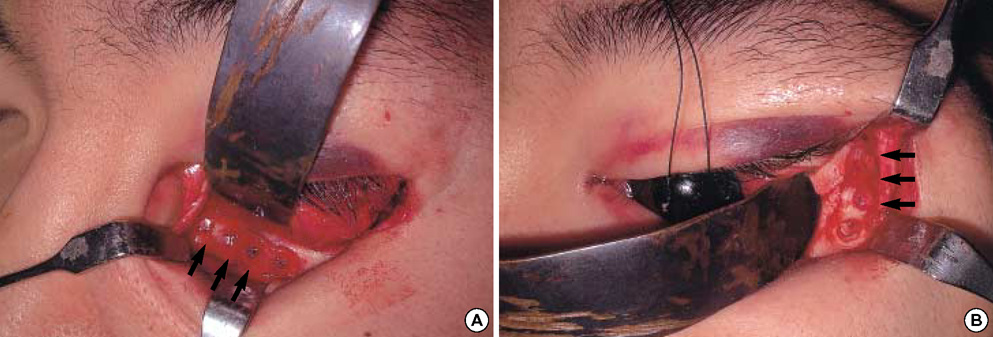
Fig. 3 Through a single transconjunctival incision, two-point fixation (inferior orbital rim and frontozygomatic suture) with four hole resorbable 2.0 mm miniplates systems (arrows) can be performed without difficulty.
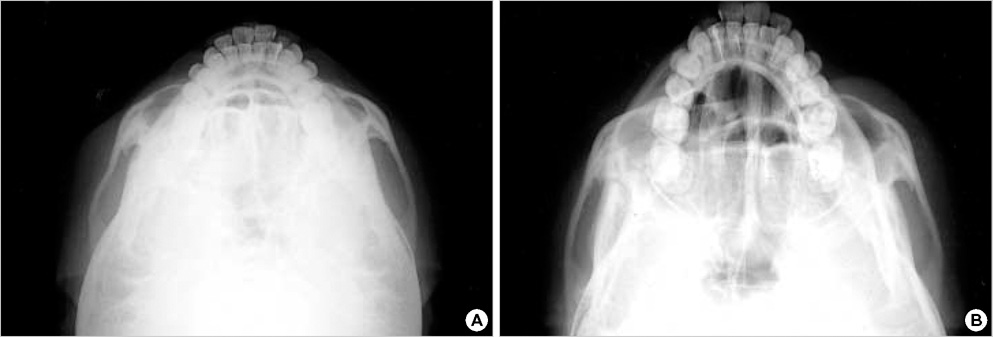
Fig. 4 (A) Preoperative zygomatic arch view (submentovertical view) shows fracture and displacement of the left zygoma bone. (B) Postoperative zygomatic arch view.
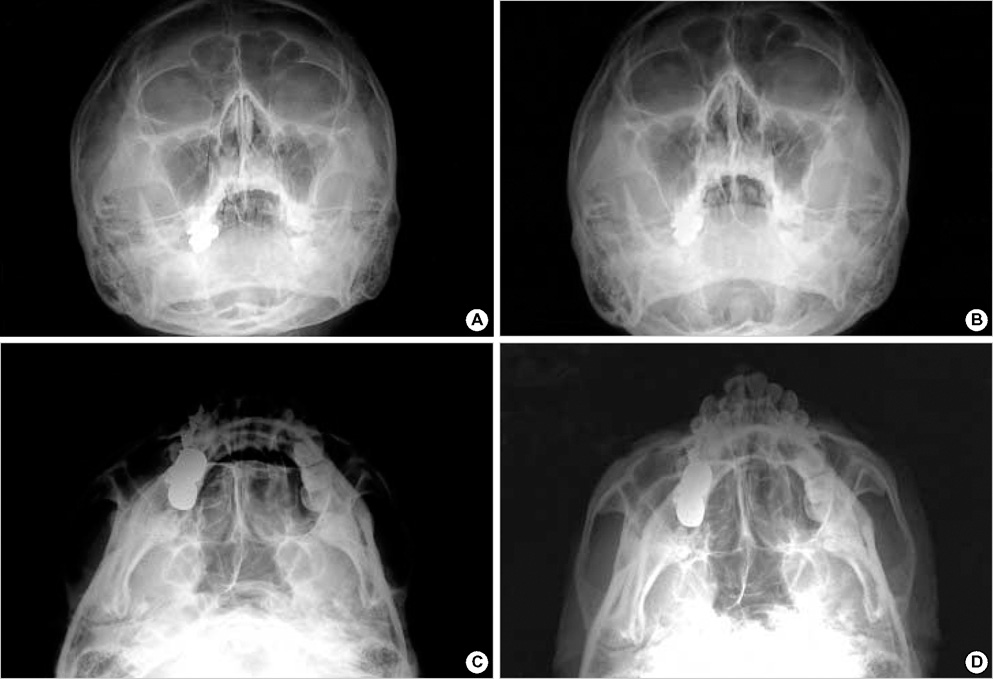
Fig. 5 (A) Preoperative skull Waters view, (B) Postoperative skull Waters view, (C) Preoperative zygomatic arch view, (D) Postoperative zygomatic arch view.
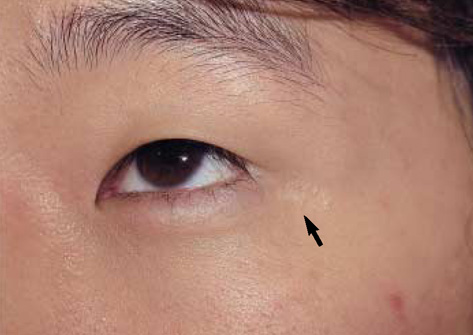
Fig. 6 Follow up at 2 yr after the operation. There is hardly visible scarring at the lateral canthal area (arrow).
Reference
-
1. Nunery WR. Lateral canthal approach to repair of trimalar fractures of the zygoma. Ophthal Plast Reconstr Surg. 1985. 1:175–183.
Article2. Tenzel RR, Miller GR. Orbital blow out fracture repair, conjunctival approach. Am J Ophthalmol. 1971. 71:1141–1142.3. Tessier P. The conjunctival approach to the orbital floor and maxilla in congenital malformation and trauma. J Maxillofac Surg. 1973. 1:3–8.
Article4. Converse JM, Firman F, Wood-Smith D. The conjunctival approach in orbital fractures. Plast Reconstr Surg. 1973. 52:656–657.
Article5. Lynch DJ, Lamp JC, Royster HP. The conjunctival approach for exploration of the orbital floor. Plast Reconstr Surg. 1974. 54:153–156.
Article6. McCord CD Jr, Moses JL. Exposure of the inferior orbit with fornix incision and lateral canthotomy. Ophthalmic Surg. 1979. 10:53–63.7. Waite PD, Carr DD. The transconjunctival approach for treating orbital trauma. J Oral Maxillofac Surg. 1991. 49:499–503.
Article8. Shaw GY, Khan J. Precise repair of orbital maxillary zygomatic fracture. Arch Otolaryngol Head Neck Surg. 1994. 120:613–619.9. Manson PN, Ruas E, Iliff N, Yaremchuk M. Single eyelid incision for exposure of the zygomatic bone and orbital reconstruction. Plast Reconstr Surg. 1987. 79:120–126.
Article10. Strong EB, Sykes JM. Zygoma complex fractures. Facial Plast Surg. 1998. 14:105–115.
Article11. Appling WD, Patrinely JR, Salzer TA. Transconjunctival approach vs subciliary skin-muscle flap approach for orbital fracture repair. Arch Otolaryngol Head Neck Surg. 1993. 119:1000–1007.
Article12. Suga H, Sugawara Y, Uda H, Kobayashi N. The transconjunctival approach for orbital bony surgery: In which cases should it be used? J Craniofac Surg. 2004. 15:454–457.
Article13. Manganello-Souza LC, de Freitas RR. Transconjunctival approach to zygomatic and orbital floor fractures. Int J Oral Maxillofac Surg. 1997. 26:31–34.
Article14. Knize DM. The superficial lateral canthal tendon:anatomic study and clinical application to lateral canthopexy. Plast Reconstr Surg. 2002. 109:1149–1157.15. Rinehart GC, Marsh JL, Hemmer KM, Bresina S. Internal fixation of malar fractures: An experimental biophysical study. Plast Reconstr Surg. 1989. 84:21–25.16. Davidson J, Nickerson D, Nickerson B. Zygomatic fractures: Comparison of method of internal fixation. Plast Reconstr Surg. 1990. 86:25–32.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 3-dimensional one point foxation with x-shaped miniplate in the cases of the zygomatic fracture
- The Significance of the Cornal incision in Treatment of Complex Zygormatic Fractures
- Surgical Methods of Zygomaticomaxillary Complex Fracture
- Transcutaneous reduction and external bone fixation device for the treatment of zygomatic arch fracture
- Endoscopically assisted reduction and rigid fixation of the zygomatic arch fracture
