Pathology of non-thermal irreversible electroporation (N-TIRE)-induced ablation of the canine brain
- Affiliations
-
- 1Department of Small Animal Clinical Sciences, Virginia-Maryland Regional College of Veterinary Medicine, Virginia Tech, Blacksburg, VA 24061, USA. jrossmei@vt.edu
- 2Bioelectromechanical Systems Laboratory, School of Biomedical Engineering and Sciences, Virginia-Tech Wake Forest University School of Biomechanical Engineering, Virginia Tech, Blacksburg, VA 24061, USA.
- 3Department of Biomedical Sciences and Pathobiology, Virginia-Maryland Regional College of Veterinary Medicine, Virginia Tech, Blacksburg, VA 24061, USA.
- 4Wake Forest University School of Medicine, Winston-Salem, NC 27157, USA.
- KMID: 1712310
- DOI: http://doi.org/10.4142/jvs.2013.14.4.433
Abstract
- This study describes the neuropathologic features of normal canine brain ablated with non-thermal irreversible electroporation (N-TIRE). The parietal cerebral cortices of four dogs were treated with N-TIRE using a dose-escalation protocol with an additional dog receiving sham treatment. Animals were allowed to recover following N-TIRE ablation and the effects of treatment were monitored with clinical and magnetic resonance imaging examinations. Brains were subjected to histopathologic and ultrastructural assessment along with Bcl-2, caspase-3, and caspase-9 immunohistochemical staining following sacrifice 72 h post-treatment. Adverse clinical effects of N-TIRE were only observed in the dog treated at the upper energy tier. MRI and neuropathologic examinations indicated that N-TIRE ablation resulted in focal regions of severe cytoarchitectural and blood-brain-barrier disruption. Lesion size correlated to the intensity of the applied electrical field. N-TIRE-induced lesions were characterized by parenchymal necrosis and hemorrhage; however, large blood vessels were preserved. A transition zone containing parenchymal edema, perivascular inflammatory cuffs, and reactive gliosis was interspersed between the necrotic focus and normal neuropil. Apoptotic labeling indices were not different between the N-TIRE-treated and control brains. This study identified N-TIRE pulse parameters that can be used to safely create circumscribed foci of brain necrosis while selectively preserving major vascular structures.
MeSH Terms
Figure
-

Fig. 1 Macroscopic morphology of non-thermal irreversible electroporation (N-TIRE) ablation in the right parietal lobe of the canine brain (Dogs 2~5). The caudal aspect of the lesion area in Dogs 2 and 3 is shown along with the rostral lesion area in Dogs 4 and 5. The right side of the brain is on the left side of the images in all panels. (A and B) Normal, pre-treatment T2W MR images. (C and D) Post-treatment T1W MR images showing a T1 iso- to hypointense lesion (white arrow). (E and F) Post-treatment T2W MR images containing focal, ovoid heterogeneously hyperintense lesions. (G and H) Post-treatment, post-contrast T1W MR images demonstrating peripheral contrast enhancement of the ablated regions. (I~L) Subgross (H&E) and gross pathologic features of brain sections corresponding to anatomic levels presented in the MR images in panels E~H. N-TIRE ablative lesions are characterized by malacia and intraparenchymal hemorrhage, and are clearly demarcated from the surrounding normal brain tissues. (M~P) Composite images generated by superimposing H&E-stained brain sections on the corresponding MRI slice. Scale bars = 1 cm (I~L).
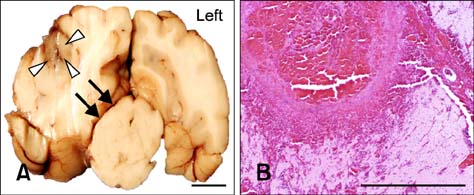
Fig. 2 Adverse effects associated with high-energy N-TIRE in Dog 5. (A) Right unilateral transtentorial herniation resulting in mesencephalic compression (black arrows) in the most caudal aspect of the N-TIRE-affected area (white arrowheads). (B) Cerebrocortical necrosis associated with marked vascular disruption and large artery thrombosis in the N-TIRE treatment region (H&E). Scale bars = 2.0 mm (B), 1cm (A).

Fig. 3 Comparative effects of N-TIRE on the superficial parietal cerebral cortex. (A) Untreated, contralateral cortex of Dog 3. (B) Sham-operated cortex demonstrating physical disruption of the neuropil by the electrode in Dog 1. (C) Collateral cortical damage extending into the adjacent neuropil in N-TIRE-affected cortex of Dog 3. H&E, Scale bars = 2.0 mm (A~C).
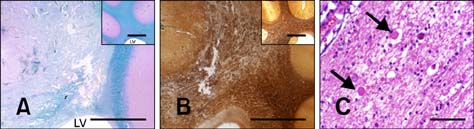
Fig. 4 Morphology of N-TIRE-induced lesions in the subcortical white matter of Dog 4. (A) Partial obliteration and vacuolization of the white matter in the corona radiata (luxol fast blue and Periodic Acid Schiff counterstain) with loss of the gray and white matter junctional distinction (inset, control). (B) Disruption of the axonal projections of the corona radiata (inset, control) of Dog 2 (Bielschowsky silver stain). (C) Vacuolar change in the white matter with axonal spheroids (arrows) in Dog 3 (H&E). LV: lateral ventricle. Scale bars = 200 µm (C), 5.0 mm (A, A inset, B and B inset).

Fig. 5 Morphology of N-TIRE-induced lesions in the deep cortical gray matter. (A) N-TIRE ablated regions (left side of panel) were sharply demarcated from the adjacent normal brain (right side) identified by their pallor. A focus of intraparenchymal hemorrhage associated with a disrupted capillary bed was visible at the lesion periphery (arrow) in Dog 2. (B) Necrotic neurons (arrowheads) and degenerate free glial nuclei in the N-TIRE-associated lesion core in Dog 4. (C) Gitter cells and intact vessels (arrows) were present in the transition zone between the affected and normal brain tissue in Dog 3. H&E. Scale bars = 200 µm (B and C inset), 500 µm (C), 2.0 mm (A).

Fig. 6 Vascular sparing effects of N-TIRE. (A) A medium sized arteriole (*) at the periphery of the N-TIRE ablation region remained intact despite diffuse damage to the surrounding neuropil in Dog 3 (H&E). (B) Electron photomicrograph of a large vessel within the core N-TIRE ablation zone of Dog 4 in which the endothelial cytoarchitecture and intravascular erythrocytes were preserved. (C) Intact vascular collagenous scaffolds in N-TIRE-treated and control (inset) gray matter of Dog 4 (trichrome). (D) CD31-positive vascular endothelial immunoreactivity and perivascular inflammation in the core N-TIRE treatment region (inset, CD31 control). (E) Electron photomicrograph of an untreated control cerebral capillary. (F) Electron photomicrographs of capillaries within the core N-TIRE ablation zone with cytoplasmic and capillary luminal disruption (*), extravasted erythrocytes, and endothelial nuclear pyknosis (inset, arrow) in Dog 2. CL: capillary lumen. Scale bars = 2 µm (E, F and F inset), 10 µm (B), 200 µm (C, C inset, D and D inset), 500 µm (A).
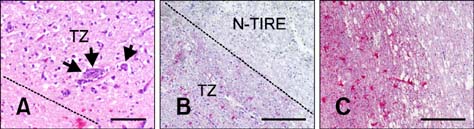
Fig. 7 N-TIRE-induced lesion transition zone (TZ). The broken gray line defines the boundary between the N-TIRE ablated region and TZ. (A) The neuropil in the TZ of Dog 2 was diffusely vacuolated and contained perviascular inflammatory cuffs (arrows; H&E). (B) An astroglial reaction in the TZ of Dog 1 (glial fibrillary acidic protein; GFAP). (C) More severe parenchymal vacuolization and astrogliosis in Dog 4 were associated with higher treatment energies (GFAP). Scale bars = 200 µm (A), 500 µm (B and C).
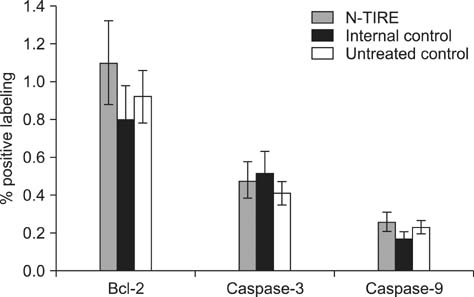
Fig. 8 Immunohistochemical evaluation of apoptosis. No differences in Bcl-2, caspase-3, and casapse-9 immunoreactivity were observed between N-TIRE-treated and control brain tissues.
Reference
-
1. Al-Sakere B, André F, Bernat C, Connault E, Opolon P, Davalos RV, Rubinsky B, Mir LM. Tumor ablation with irreversible electroporation. PLoS One. 2007; 2:e1135.
Article2. Atsumi H, Matsumae M, Kaneda M, Muro I, Mamata Y, Komiya T, Tsugu A, Tsugane R. Novel laser system and laser irradiation method reduced the risk of carbonization during laser interstitial thermotherapy: assessed by MR temperature measurement. Lasers Surg Med. 2001; 29:108–117.
Article3. Chen LQ, Wei JS, Lei ZN, Zhang LM, Liu Y, Sun FY. Induction of Bcl-2 and Bax was related to hyperphosphorylation of tau and neuronal death induced by okadaic acid in rat brain. Anat Rec A Discov Mol Cell Evol Biol. 2005; 287:1236–1245.
Article4. Chizmadzhev YA, Zarnitsin VG, Weaver JC, Potts RO. Mechanism of electroinduced ionic species transport through a multilamellar lipid system. Biophys J. 1995; 68:749–765.
Article5. Cosman ER, Nashold BS, Bedenbaugh P. Stereotactic radiofrequency lesion making. Appl Neurophysiol. 1983; 46:160–166.
Article6. Davalos RV, Mir LM, Rubinsky B. Tissue ablation with irreversible electroporation. Ann Biomed Eng. 2005; 33:223–231.
Article7. Dev SB, Hofmann GA. Electrochemotherapy-a novel method of cancer treatment. Cancer Treat Rev. 1994; 20:105–115.
Article8. Edd JF, Horowitz L, Davalos RV, Mir LM, Rubinsky B. In vivo results of a new focal tissue ablation technique: irreversible electroporation. IEEE Trans Biomed Eng. 2006; 53:1409–1415.
Article9. Ellis TL, Garcia PA, Rossmeisl JH Jr, Henao-Guerrero N, Robertson J, Davalos RV. Nonthermal irreversible electroporation for intracranial surgical applications. J Neurosurg. 2011; 114:681–688.
Article10. Esiri M, Squier W, Perl D. Oppenheimer's Diagnostic Neuropathology: A Practical Manual. 3rd ed. Boca Raton: CRC Press;2006. p. 531–537.11. Foster RS, Bihrle R, Sanghvi NT, Fry FJ, Donohue JP. High-intensity focused ultrasound in the treatment of prostatic disease. Eur Urol. 1993; 23:Suppl 1. 29–33.
Article12. Garcia PA, Pancotto TE, Rossmeisl JH Jr, Henao-Guerrero N, Gustafson NR, Daniel GB, Robertson JL, Ellis TL, Davalos RV. Non-thermal irreversible electroporation (N-TIRE) and adjuvant fractionated radiotherapeutic multimodal therapy for intracranial malignant glioma in a canine patient. Technol Cancer Res Treat. 2011; 10:73–83.
Article13. Garcia PA, Rossmeisl JH Jr, Neal RE II, Ellis TL, Olson JD, Henao-Guerreo N, Robertson J, Davalos RV. Intracranial nonthermal irreversible electroporation: in vivo analysis. J Membr Biol. 2010; 236:127–136.14. Lee EW, Loh CT, Kee ST. Imaging guided percutaneous irreversible electroporation: ultrasound and immunohistological correlation. Technol Cancer Res Treat. 2007; 6:287–294.
Article15. Maor E, Ivorra A, Leor J, Rubinsky B. The effect of irreversible electroporation on blood vessels. Technol Cancer Res Treat. 2007; 6:307–312.
Article16. Miklavčič D, Šemrov D, Mekid H, Mir LM. A validated model of in vivo electric field distribution in tissues for electrochemotherapy and for DNA electrotransfer for gene therapy. Biochim Biophys Acta. 2000; 1523:73–83.
Article17. National Research Council. Guide for the Care and Use of Laboratory Animals. 8th ed. Washington: The National Academies Press;2011. p. 11–124.18. Onik G, Mikus P, Rubinsky B. Irreversible electroporation: implications for prostate ablation. Technol Cancer Res Treat. 2007; 6:295–300.
Article19. Rubinsky B. Irreversible electroporation in medicine. Technol Cancer Res Treat. 2007; 6:255–260.
Article20. Rubinsky B, Onik G, Mikus P. Irreversible electroporation: a new ablation modality-clinical implications. Technol Cancer Res Treat. 2007; 6:37–48.
Article21. Shafiee H, Garcia PA, Davalos RV. A preliminary study to delineate irreversible electroporation from thermal damage using the arrhenius equation. J Biomech Eng. 2009; 131:074509.
Article22. Tacke J. Thermal therapies in interventional MR imaging. Cryotherapy. Neuroimaging Clin N Am. 2001; 11:759–765.23. Weaver JC. Electroporation: a general phenomenon for manipulating cells and tissues. J Cell Biochem. 1993; 51:426–435.
Article24. Yakovlev AG, Faden AI. Mechanisms of neural cell death: implications for development of neuroprotective treatment strategies. NeuroRx. 2004; 1:5–16.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Irreversible electroporation of hepatocellular carcinoma: the role of ultrasonography
- Irreversible Electroporation: A Novel Image-Guided Cancer Therapy
- Current Research Status of Irreversible Electroporation for Hollow Viscus Organ of Gastrointestinal Tract
- Irreversible Electroporation of a Hepatocellular Carcinoma Lesion Adjacent to a Transjugular Intrahepatic Portosystemic Shunt Stent Graft
- Irreversible electroporation for the treatment of pancreatic neuroendocrine tumors
