Bone Positron Emission Tomography with or without CT Is More Accurate than Bone Scan for Detection of Bone Metastasis
- Affiliations
-
- 1Department of Nuclear Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 463-707, Korea. wwlee@snu.ac.kr
- 2Institute of Radiation Medicine, Medical Research Center, Seoul National University, Seoul 110-744, Korea.
- KMID: 1705468
- DOI: http://doi.org/10.3348/kjr.2013.14.3.510
Abstract
OBJECTIVE
Na18F bone positron emission tomography (bone PET) is a new imaging modality which is useful for the evaluation of bone diseases. Here, we compared the diagnostic accuracies between bone PET and bone scan for the detection of bone metastasis (BM).
MATERIALS AND METHODS
Sixteen cancer patients (M:F = 10:6, mean age = 60 +/- 12 years) who underwent both bone PET and bone scan were analyzed. Bone PET was conducted 30 minutes after the injection of 370 MBq Na18F, and a bone scan was performed 3 hours after the injection of 1295 MBq 99mTc-hydroxymethylene diphosphonate.
RESULTS
In the patient-based analysis (8 patients with BM and 8 without BM), the sensitivities of bone PET (100% = 8/8) and bone scan (87.5% = 7/8) were not significantly different (p > 0.05), whereas the specificity of bone PET (87.5% = 7/8) was significantly greater than that of the bone scan (25% = 2/8) (p < 0.05). In the lesion-based analysis (43 lesions in 14 patients; 31 malignant and 12 benign), the sensitivity of bone PET (100% = 31/31) was significantly greater than that of bone scan (38.7% = 12/31) (p < 0.01), and the specificity of bone PET (75.0% = 9/12) was also significantly higher than that of bone scan (8.3% = 1/12) (p < 0.05). The receiver operating characteristic curve analysis showed that bone PET was significantly more accurate than the bone scan in the patient (p = 0.0306) and lesion (p = 0.0001) based analyses.
CONCLUSION
Na18F bone PET is more accurate than bone scan for BM evaluation.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Area Under Curve
Bone Neoplasms/*radionuclide imaging/*secondary
Diphosphonates/diagnostic use
Female
Fluorine Radioisotopes/diagnostic use
Fluorodeoxyglucose F18/diagnostic use
Humans
Male
Middle Aged
Multimodal Imaging/methods
Organotechnetium Compounds/diagnostic use
Positron-Emission Tomography/*methods
Retrospective Studies
Sensitivity and Specificity
Sodium/diagnostic use
Tomography, X-Ray Computed/methods
Diphosphonates
Fluorine Radioisotopes
Fluorodeoxyglucose F18
Organotechnetium Compounds
Sodium
Figure
-

Fig. 1 Findings of bone positron emission tomography (PET) and bone scan in 84-year-old male prostate cancer patient (no.2 in Table 1) with numerous bone metastatic lesions. A. Anterior and posterior planar images of bone scan show multiple bone metastases. B. Bone PET anterior and posterior maximum-intensity projection images reveal numerous metasatic bone leisons. Please note that metastatic lesions on bone PET are more prominent than those on bone scan.

Fig. 2 Case demonstration showing higher specificity of bone positron emission tomography (PET) than bone scan in 77-year-old male patient with colon cancer (no.14 in Table 1). He has been complaining of intractable back pain. A. Bone scan shows focally increased uptake at L4 vertebral body (black arrows), which was suspected of bone metastasis. B. Bone PET maximum-intensity projection images also revealed hot uptake at same location (black arrows). C. Trans-axial images of CT, bone PET, and fusion image (from left to right) clearly demonstrate that osteophyte at L4 has intense uptake of Na18F (white arrow). It is noteworthy that tomographic images (C) play decisive role in determining nature of osteophyte.
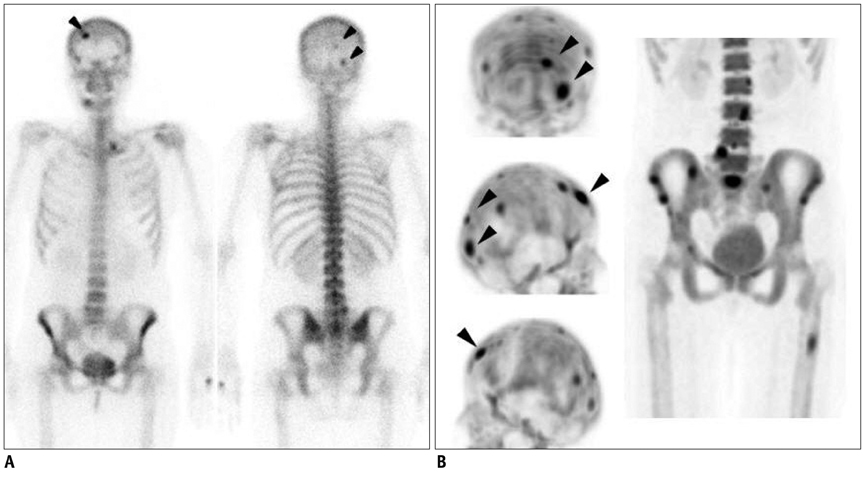
Fig. 3 Case demonstration showing higher sensitivity of bone positron emission tomography (PET) than bone scan in 44-year-old female patient with breast cancer (no.3 in Table 1). A. Anterior and posterior bone scan images show only 3 abnormal foci in skull (arrowheads). B. Skull lesions observed in bone scan are found to be more prominent in bone PET (arrowheads) (top, posterior maximum-intensity projection [MIP]; middle, right lateral MIP; and bottom, left lateral MIP images). In addition, many other bone metastatic lesions are found in skull, lumbar spines, sacrum, pelvic bones, and left femur.
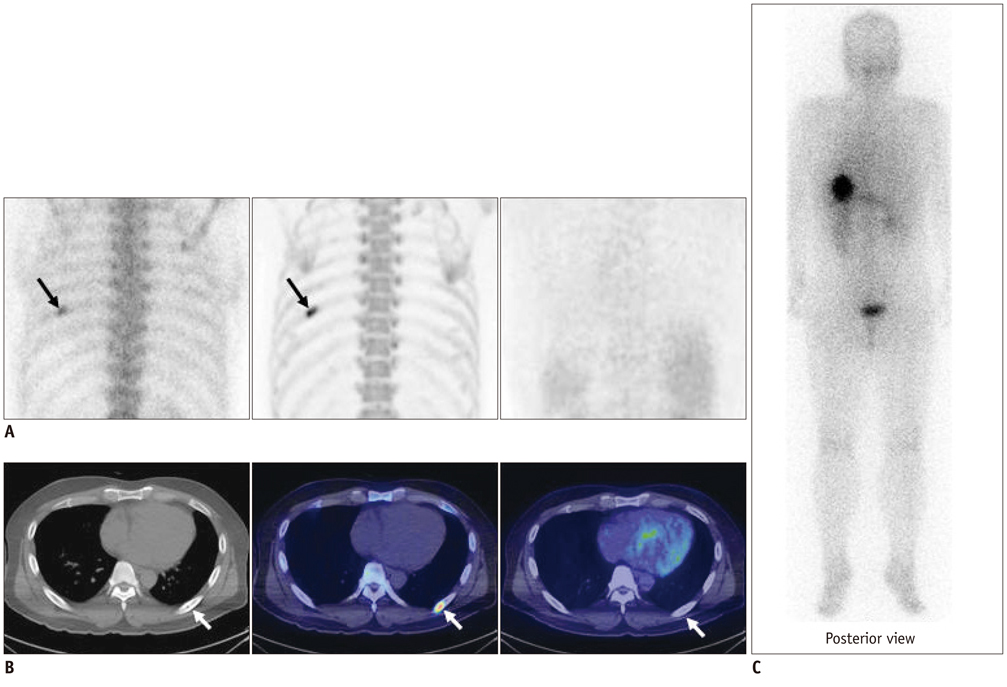
Fig. 4 Case demonstration showing false positivity of bone positron emission tomography (PET) and bone scan in 39-year-old male patient with thyroid cancer (no.9 in Table 1). A. (left, bone scan posterior planar; middle, bone PET posterior maximum-intensity projection [MIP]; and right, 18F-FDG PET posterior image) Bone scan and bone PET revealed abnormal uptake in left 7th rib posterior arc (black arrows); however, 18F-FDG PET was negative in left 7th rib area. B. (left, CT; middle, fusion of bone PET/CT; and right, fusion of 18F-FDG PET/CT) CT revealed osteosclerotic lesion in left 7th rib posterior arc, which was compatible with hot uptake in bone PET/CT; however, lesion was negative in 18F-FDG PET/CT (white arrows). C. Posterior image of 131I whole body scan obtained 2 days after administration of 131I (30 mCi). No lesion was found in left 7th rib area.

Fig. 5 Receiver operating characteristic curve analyses. Bone positron emission tomography (PET) was significantly more accurate than bone scan in patient (p = 0.0306) and lesion (p = 0.0001) based analyses.
Reference
-
1. Grant FD, Fahey FH, Packard AB, Davis RT, Alavi A, Treves ST. Skeletal PET with 18F-fluoride: applying new technology to an old tracer. J Nucl Med. 2008. 49:68–78.2. Iagaru A, Mittra E, Dick DW, Gambhir SS. Prospective evaluation of (99m)Tc MDP scintigraphy, (18)F NaF PET/CT, and (18)F FDG PET/CT for detection of skeletal metastases. Mol Imaging Biol. 2012. 14:252–259.3. Hoh CK, Hawkins RA, Dahlbom M, Glaspy JA, Seeger LL, Choi Y, et al. Whole body skeletal imaging with [18F]fluoride ion and PET. J Comput Assist Tomogr. 1993. 17:34–41.4. Czernin J, Satyamurthy N, Schiepers C. Molecular mechanisms of bone 18F-NaF deposition. J Nucl Med. 2010. 51:1826–1829.5. Blau M, Nagler W, Bender MA. Fluorine-18: a new isotope for bone scanning. J Nucl Med. 1962. 3:332–334.6. Thrall JH. Technetium-99m labeled agents for skeletal imaging. CRC Crit Rev Clin Radiol Nucl Med. 1976. 8:1–31.7. Hawkins RA, Choi Y, Huang SC, Hoh CK, Dahlbom M, Schiepers C, et al. Evaluation of the skeletal kinetics of fluorine-18-fluoride ion with PET. J Nucl Med. 1992. 33:633–642.8. Schirrmeister H, Guhlmann A, Elsner K, Kotzerke J, Glatting G, Rentschler M, et al. Sensitivity in detecting osseous lesions depends on anatomic localization: planar bone scintigraphy versus 18F PET. J Nucl Med. 1999. 40:1623–1629.9. Schirrmeister H, Glatting G, Hetzel J, Nüssle K, Arslandemir C, Buck AK, et al. Prospective evaluation of the clinical value of planar bone scans, SPECT, and (18)F-labeled NaF PET in newly diagnosed lung cancer. J Nucl Med. 2001. 42:1800–1804.10. Hetzel M, Arslandemir C, König HH, Buck AK, Nüssle K, Glatting G, et al. F-18 NaF PET for detection of bone metastases in lung cancer: accuracy, cost-effectiveness, and impact on patient management. J Bone Miner Res. 2003. 18:2206–2214.11. Messa C, Goodman WG, Hoh CK, Choi Y, Nissenson AR, Salusky IB, et al. Bone metabolic activity measured with positron emission tomography and [18F]fluoride ion in renal osteodystrophy: correlation with bone histomorphometry. J Clin Endocrinol Metab. 1993. 77:949–955.12. Installé J, Nzeusseu A, Bol A, Depresseux G, Devogelaer JP, Lonneux M. (18)F-fluoride PET for monitoring therapeutic response in Paget's disease of bone. J Nucl Med. 2005. 46:1650–1658.13. Uchida K, Nakajima H, Miyazaki T, Yayama T, Kawahara H, Kobayashi S, et al. Effects of alendronate on bone metabolism in glucocorticoid-induced osteoporosis measured by 18F-fluoride PET: a prospective study. J Nucl Med. 2009. 50:1808–1814.14. Kang JY, Lee WW, So Y, Lee BC, Kim SE. Clinical Usefulness of 18F-fluoride Bone PET. Nucl Med Mol Imaging. 2010. 44:55–61.15. Even-Sapir E. Imaging of malignant bone involvement by morphologic, scintigraphic, and hybrid modalities. J Nucl Med. 2005. 46:1356–1367.16. Even-Sapir E, Metser U, Mishani E, Lievshitz G, Lerman H, Leibovitch I. The detection of bone metastases in patients with high-risk prostate cancer: 99mTc-MDP Planar bone scintigraphy, single- and multi-field-of-view SPECT, 18F-fluoride PET, and 18F-fluoride PET/CT. J Nucl Med. 2006. 47:287–297.17. Schirrmeister H, Guhlmann A, Kotzerke J, Santjohanser C, Kühn T, Kreienberg R, et al. Early detection and accurate description of extent of metastatic bone disease in breast cancer with fluoride ion and positron emission tomography. J Clin Oncol. 1999. 17:2381–2389.18. Schiepers C, Nuyts J, Bormans G, Dequeker J, Bouillon R, Mortelmans L, et al. Fluoride kinetics of the axial skeleton measured in vivo with fluorine-18-fluoride PET. J Nucl Med. 1997. 38:1970–1976.19. Cook GJ, Blake GM, Marsden PK, Cronin B, Fogelman I. Quantification of skeletal kinetic indices in Paget's disease using dynamic 18F-fluoride positron emission tomography. J Bone Miner Res. 2002. 17:854–859.20. Uematsu T, Yuen S, Yukisawa S, Aramaki T, Morimoto N, Endo M, et al. Comparison of FDG PET and SPECT for detection of bone metastases in breast cancer. AJR Am J Roentgenol. 2005. 184:1266–1273.21. Ito S, Kato K, Ikeda M, Iwano S, Makino N, Tadokoro M, et al. Comparison of 18F-FDG PET and bone scintigraphy in detection of bone metastases of thyroid cancer. J Nucl Med. 2007. 48:889–895.22. Langsteger W, Heinisch M, Fogelman I. The role of fluorodeoxyglucose, 18F-dihydroxyphenylalanine, 18F-choline, and 18F-fluoride in bone imaging with emphasis on prostate and breast. Semin Nucl Med. 2006. 36:73–92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nuclear Medicine Imaging in Rheumatic Diseases
- F-18 Sodium Fluoride Positron Emission Tomography/Computed Tomography for Detection of Thyroid Cancer Bone Metastasis Compared with Bone Scintigraphy
- Discrepancy of Bone Metastases between F-18 FDG PET/CT and Bone Scan in a Patient with Prostate Cancer
- Orbital Rim Uptake on Bone Scans and Its Clinical Significance
- Efficiency of Positron Emission Tomography (PET) in Diagnosis of Breast Cancer
