Korean J Gastroenterol.
2013 May;61(5):279-281. 10.4166/kjg.2013.61.5.279.
A Case of Dieulafoy Lesion of the Jejunum Presented with Massive Hemorrhage
- Affiliations
-
- 1Department of Internal Medicine, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea. bkpark@nhimc.or.kr
- 2Department of Diagnostic Radiology, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea.
- 3Department of General Surgery, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea.
- 4Department of Pathology, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea.
- KMID: 1501650
- DOI: http://doi.org/10.4166/kjg.2013.61.5.279
Abstract
- The Dieulafoy lesion is a rare cause of severe gastrointestinal hemorrhage. Although it may occur anywhere in the gastrointestinal tract, the lesion is most commonly located in the stomach, and the small bowel is an extremely uncommon site. Since Dieulafoy lesion in the small bowel is difficult to access by endoscopy, it seems impossible to diagnose and treat by initial endoscopy unlike the lesions in stomach. We experienced a case of Dieulafoy lesion of jejunum with massive hemorrhage in 54-year-old male. Active jejunal bleeding was shown by computed tomography scan and mesenteric angiography. Partial resection of the jejunum was performed. Final pathologic finding revealed Dieulafoy lesion of the jejunum.
MeSH Terms
Figure
-
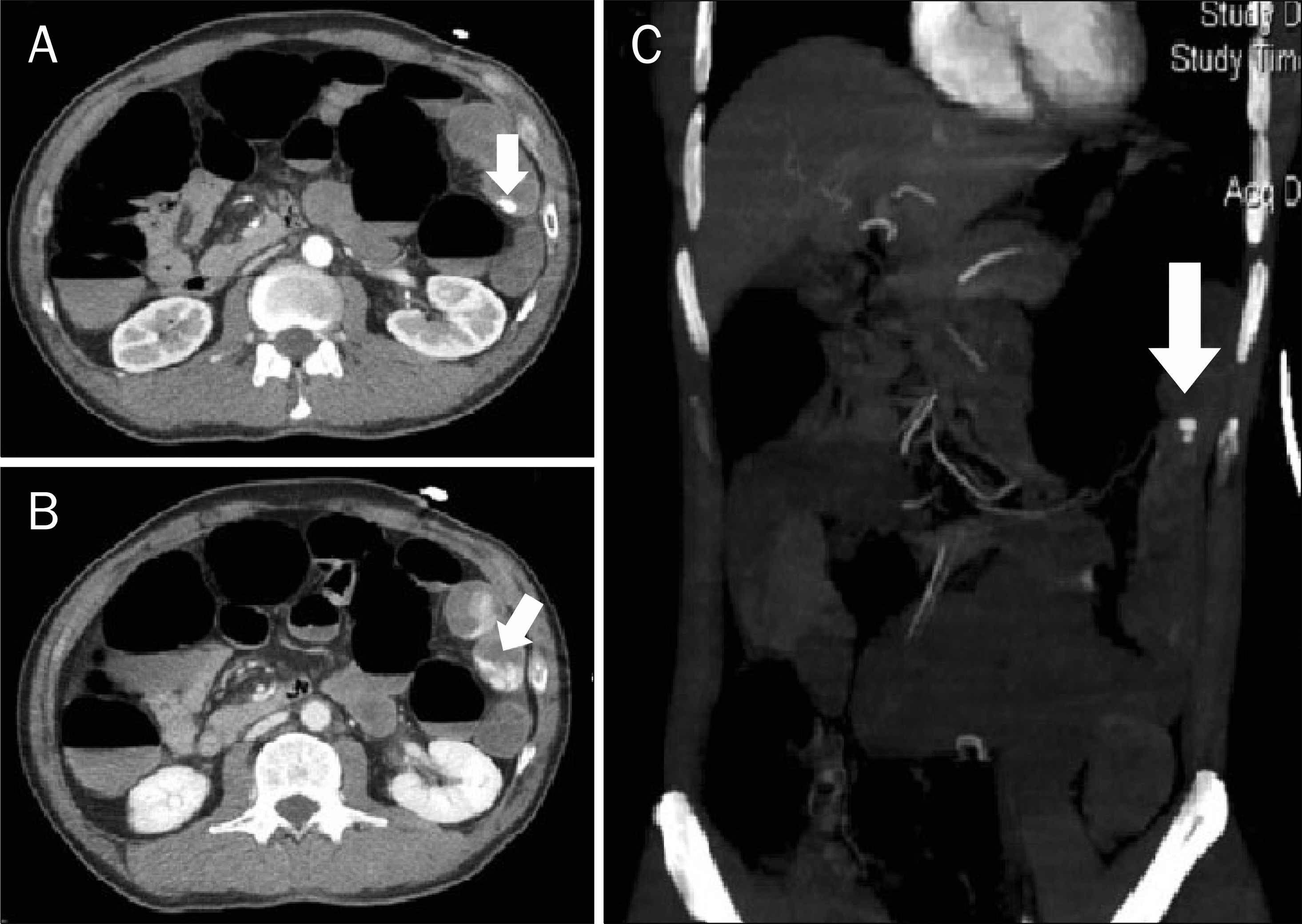
Fig. 1. Axial section of CT scan showing bleeding focus in the jejunum (arrow) at arterial phase (A), and contrast leakage into jejunum (arrow) at venous phase (B). (C) CT angiography showing arterial bleeding on jejunum (arrow).
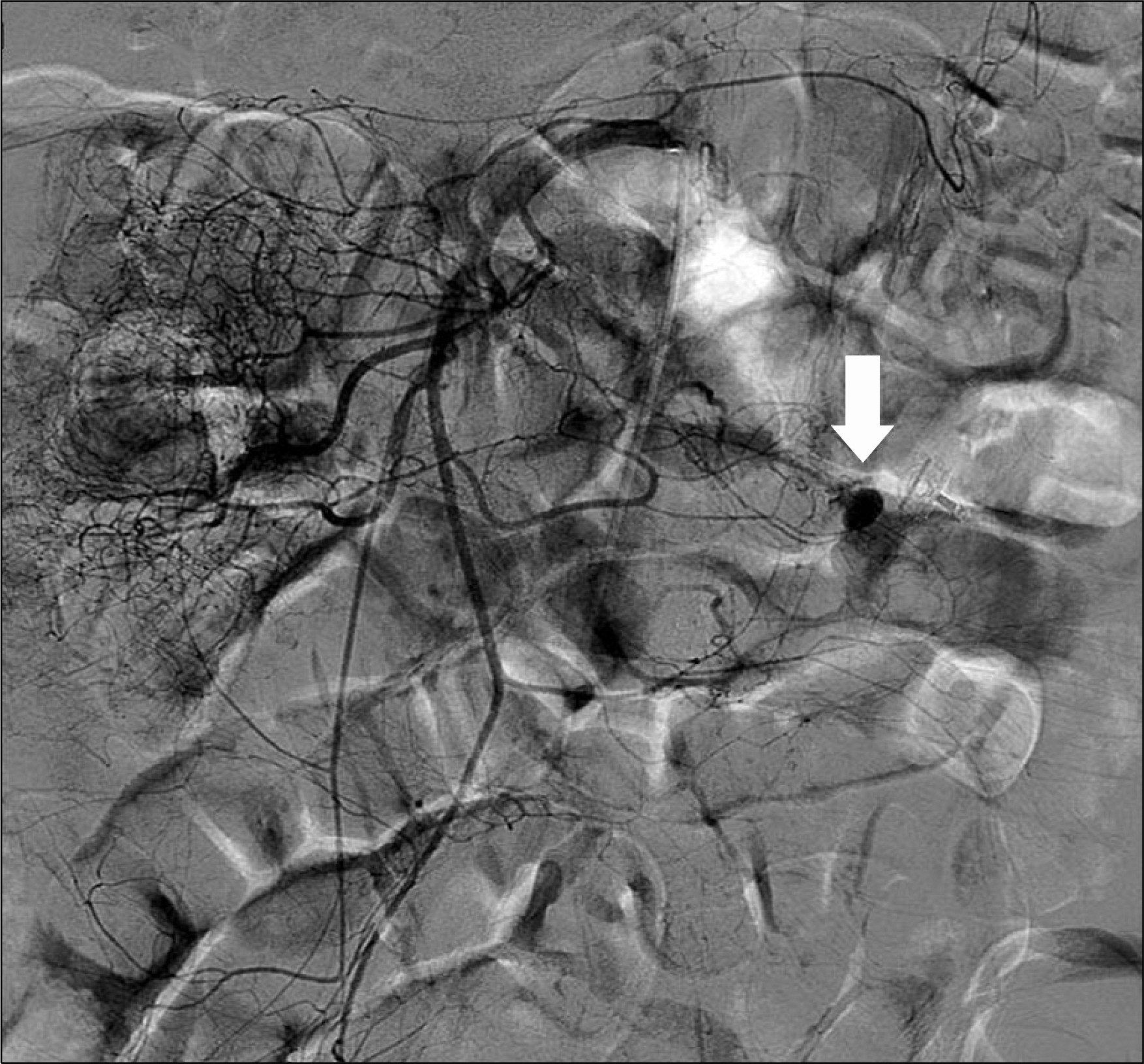
Fig. 2. Mesenteric angiography showed ectatic artery accompanied by contrast extravasation and staining (arrow) at the jejunum level.

Fig. 3. A microscopic finding of resected bowel specimen showed erosive mucosa in contact with a large tortuous submucosal vessel filled with thrombi (H&E, ×125).
Reference
-
References
1. Veldhuyzen van Zanten SJ, Bartelsman JF, Schipper ME, Tytgat GN. Recurrent massive haematemesis from Dieulafoy vascular malformations–a review of 101 cases. Gut. 1986; 27:213–222.
Article2. Schmulewitz N, Baillie J. Dieulafoy lesions: a review of 6 years of experience at a tertiary referral center. Am J Gastroenterol. 2001; 96:1688–1694.
Article3. Blecker D, Bansal M, Zimmerman RL, et al. Dieulafoy's lesion of the small bowel causing massive gastrointestinal bleeding: two case reports and literature review. Am J Gastroenterol. 2001; 96:902–905.
Article4. Kim JK, Jo BJ, Lee KM, et al. Dieulafoy's lesion of jejunum: presenting small bowel mass and stricture. Yonsei Med J. 2005; 46:445–447.
Article5. Chaer RA, Helton WS. Dieulafoy's disease. J Am Coll Surg. 2003; 196:290–296.
Article6. Juler GL, Labitzke HG, Lamb R, Allen R. The pathogenesis of Dieulafoy's gastric erosion. Am J Gastroenterol. 1984; 79:195–200.7. Lee YT, Walmsley RS, Leong RW, Sung JJ. Dieulafoy's lesion. Gastrointest Endosc. 2003; 58:236–243.
Article8. Baxter M, Aly EH. Dieulafoy's lesion: current trends in diagnosis and management. Ann R Coll Surg Engl. 2010; 92:548–554.
Article9. Durham JD, Kumpe DA, Rothbarth LJ, Van Stiegmann G. Dieulafoy disease: arteriographic findings and treatment. Radiology. 1990; 174:937–941.
Article10. Defreyne L, Vanlangenhove P, De Vos M, et al. Embolization as a first approach with endoscopically unmanageable acute non-variceal gastrointestinal hemorrhage. Radiology. 2001; 218:739–748.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dieulafoy - like Lesions of Nontraditional Locations in Gastric Antrum and Jejunum
- A Case of a Jejunal Dieulafoy's Lesion Mimicking a Submucosal Tumor
- Two Cases of Rectal Dieulafoy's Lesion with Massive Hematochezia in Elderly Patients
- A Case of Dieulafoy's Lesion in the Jejunum Treated by Double Balloon Enteroscopy
- An Incidental Asymptomatic Dieulafoy's Lesion in the Colon: A Case Report
