Selection and Recommended Usage Guide of Temporary External Fixator
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. limsj@skku.edu
- 2Department of Orthopedic Surgery, Kyungpook National University Hospital, Kyungpook National University Medical School, Daegu, Korea.
- KMID: 1496173
- DOI: http://doi.org/10.12671/jkfs.2013.26.2.164
Abstract
- No abstract available.
MeSH Terms
Figure
-

Fig. 1 (A) A 19-year-old female patient was referred to our hospital with proximal tibial segmental fracture spanned with a knee-spanning external fixator. (B) Poorly placed tibial pins violating future incision area for internal fixation, as well as providing no stability to the tibial shaft fracture. Mild ischemic changes were also noted due to compromised blood supply. (C, D) After converting to plating, deep infection developed at the original half pin site, finally resulting in osteomyelitis.

Fig. 2 (A) A 59-year-old female patient was referred to our hospital with open distal femoral comminuted fracture stabilized with a knee-spanning frame. Anterior femoral pins were placed away from anticipated lateral incision, but overlapped with planned plating position. (B) Pin site debridement was performed along with administration of antibiotics for 1 week, and then definitive surgery was performed. (C) One year after surgery, union was obtained with no sign of infection.
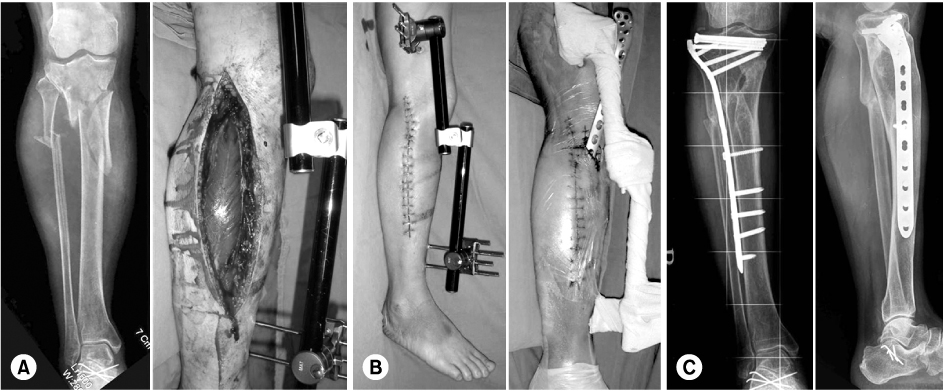
Fig. 3 (A) Tibial plateau fracture was stabilized with a knee-spanning external fixator after a single incision fasciotomy. (B) Note the placement of lateral femoral pins to avoid violating quadriceps mechanism. At 14 days, the fracture was stabilized with minimally invasive percutaneous plating. (C) One year after surgery, union was obtained with no sign of infection.
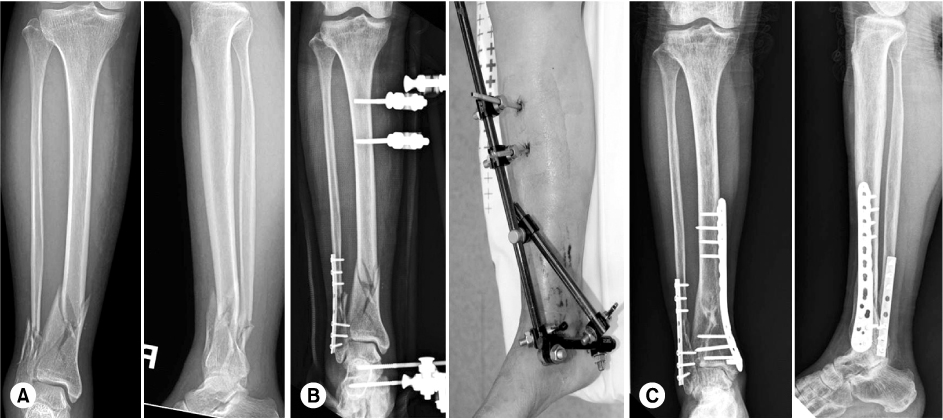
Fig. 4 (A) A 53-year-old female patient sustaining a comminuted tibial pilon fracture. (B) She was treated acutely with open plating of comminuted fibular fracture and an ankle-spanning monolateral external fixator. (C) Tibial pilon fracture was stabilized with percutaneous medial plating and healed with no infection or wound problem at 1 year after the surgery.

Fig. 5 (A) A 69-year-old female patient sustaining a tibial pilon fracture with hemorrhagic fracture blisters. (B) The fracture was stabilized with an ankle-spanning external fixator of delta configuration. (C) After healing of soft tissue at 14 days, definitive stabilization was performed with open plating for fibular fracture and percutaneous medial plating for tibial pilon fracture.
Reference
-
1. Anglen JO. Early outcome of hybrid external fixation for fracture of the distal tibia. J Orthop Trauma. 1999. 13:92–97.
Article2. Anglen JO, Aleto T. Temporary transarticular external fixation of the knee and ankle. J Orthop Trauma. 1998. 12:431–434.
Article3. Barei DP, Nork SE, Mills WJ, Henley MB, Benirschke SK. Complications associated with internal fixation of high-energy bicondylar tibial plateau fractures utilizing a two-incision technique. J Orthop Trauma. 2004. 18:649–657.
Article4. Behrens F. General theory and principles of external fixation. Clin Orthop Relat Res. 1989. (241):15–23.
Article5. Blauth M, Bastian L, Krettek C, Knop C, Evans S. Surgical options for the treatment of severe tibial pilon fractures: a study of three techniques. J Orthop Trauma. 2001. 15:153–160.
Article6. Casey D, McConnell T, Parekh S, Tornetta P 3rd. Percutaneous pin placement in the medial calcaneus: is anywhere safe? J Orthop Trauma. 2002. 16:26–29.
Article7. Chen SH, Wu PH, Lee YS. Long-term results of pilon fractures. Arch Orthop Trauma Surg. 2007. 127:55–60.
Article8. Collinge C, Kennedy J, Schmidt A. Temporizing external fixation of the lower extremity: a survey of the Orthopaedic Trauma Association Membership. Orthopedics. 2010. 239–244. [Epub ahead of print].
Article9. Dillin L, Slabaugh P. Delayed wound healing, infection, and nonunion following open reduction and internal fixation of tibial plafond fractures. J Trauma. 1986. 26:1116–1119.
Article10. Haidukewych GJ. Temporary external fixation for the management of complex intra- and periarticular fractures of the lower extremity. J Orthop Trauma. 2002. 16:678–685.
Article11. Lau TW, Leung F, Chan CF, Chow SP. Wound complication of minimally invasive plate osteosynthesis in distal tibia fractures. Int Orthop. 2008. 32:697–703.
Article12. Oh CW, Lee HJ. Acute compartment syndrome after trauma. J Korean Fract Soc. 2010. 23:399–403.
Article13. Oh JK, Hwang JH, Sahu D, Jun SH. Complication rate and pitfalls of temporary bridging external fixator in periarticular communited fractures. Clin Orthop Surg. 2011. 3:62–68.
Article14. Patterson MJ, Cole JD. Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma. 1999. 13:85–91.
Article15. Phisitkul P, McKinley TO, Nepola JV, Marsh JL. Complications of locking plate fixation in complex proximal tibia injuries. J Orthop Trauma. 2007. 21:83–91.
Article16. Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr. A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma. 2004. 18:S32–S38.
Article17. Sohn OJ, Kang DH. Staged protocol in treatment of open distal tibia fracture: using lateral MIPO. Clin Orthop Surg. 2011. 3:69–76.
Article18. Watson JT, Moed BR, Karges DE, Cramer KE. Pilon fractures. Treatment protocol based on severity of soft tissue injury. Clin Orthop Relat Res. 2000. (375):78–90.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Staged Treatment of Bicondylar Tibial Plateau Fracture (Schatzker Type V or VI) Using Temporary External Fixator: Correlation between Clinical and Radiological Outcomes
- Cross-Leg Flap Imobilized with External Fixator Brace
- Rupture of Femoral Artery by External Fixator
- A Clinical Analysis on Treatment of Tibial Fractures Using Ex-Fi-Re External Fixator
- Treatment of Wrist Frarture-Disluation using the Mini-External Fixator and Internal Fixation
