The Efficacy and Long-Term Outcome of Microcoil Embolotherapy for Acute Lower Gastrointestinal Bleeding
- Affiliations
-
- 1Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung 813, Taiwan. hlliang@vghks.gov.tw
- 2Department of Radiology, Kaohsiung National Yang-Ming University, Taipei 112, Taiwan.
- KMID: 1482785
- DOI: http://doi.org/10.3348/kjr.2013.14.2.259
Abstract
OBJECTIVE
To evaluate the clinical efficacy as well as long-term clinical outcomes of superselective microcoil embolization for lower gastrointestinal bleeding (LGIB).
MATERIALS AND METHODS
Between 1997 and 2009, 26 patients with intended transcatheter embolotherapy for LGIB were retrospectively reviewed. Embolization was performed only when the catheter could be advanced to or distal to the mesenteric border of the bowel. The main purpose of our study was to assess technical success, recurrent bleeding rate and complications. We also evaluated the long-term clinical outcome, including late recurrent LGIB, bowel ischemia and the survival rate.
RESULTS
Twenty-two bleeding sources were in the territory of superior mesenteric artery and four in the inferior mesenteric artery. Technical success was achieved in 22 patients (84.6%). The target vessel of embolization was vasa recta in seventeen patients and marginal artery in the remaining five patients. Early rebleeding occurred in two patients (7.7%) and bowel ischemia in two patients, of whom the embolized points were both at the marginal artery. Delayed recurrent bleeding (> 30 days) occurred in two angiodysplasia patients. Five patients (19.2%) died within the first 30 days of intervention. Long-term follow-up depicted estimated survival rates of 58.2 and 43.1% after one, and five years, respectively.
CONCLUSION
Transcatheter embolotherapy to treat LGIB is effective with low rebleeding and ischemic complications. Considering the advanced age and complex medical problems of these patients, the minimal invasive embolotherapy may be used as both a primary and potentially definitive treatment of LGIB.
MeSH Terms
Figure
-

Fig. 1 36-year-old man with bleeding jejuna ulcer. A. CT angiography showing contrast extravasation (arrow), indicating active bleeding in the jejunum. B. Confirmation of contrast extravasation (arrow) in jejunum based on superior mesenteric artery angiogram. C. Bowel had moved to left upper abdomen during superselective catheterization. Arrow: contrast extravasation. D. Two straight microcoils (arrow) were placed in vasa recta. Immediate follow-up angiogram revealed no residual contrast extravasation. Patient is uneventful without recurrent lower gastrointestinal bleeding until end of study for 72-month follow up.
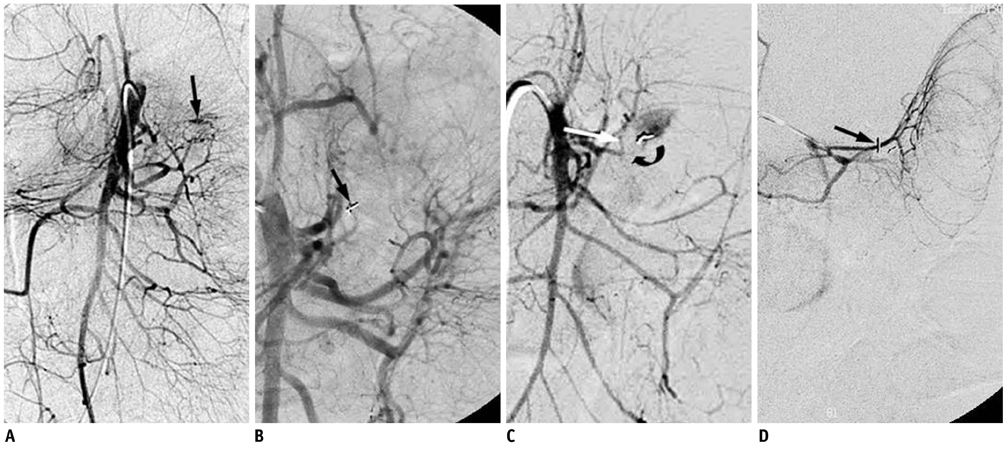
Fig. 2 61-year-old female with corrosive injury post gastrectomy. A. Superior meaenteric artery angiogram showing contrast extravasation (arrow) at proximal jejunum. B. After straight microcoils (arrow) embolization, no residual contrast extravasation on follow-up angiogram can be identified. C. Recurrent bleeding occurred 7 days after initial successful embolization. SMA angiogram showing contrast extravasation from another vasa recta branch (arrow). Previously embolized branch was occluded (curved arrow). D. After another microcoils embolization (arrow), no residual contrast extravasation can be identified on follow-up angiogram. No recurrent bleeding occurred in this patient, but unfortunately patient died due to multi-organ failure 1.5 months later.
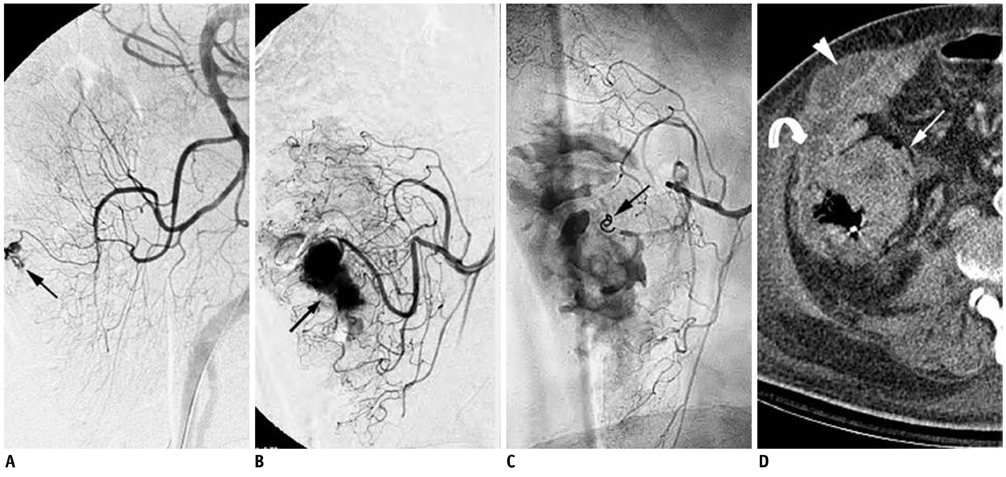
Fig. 3 66-year-old man with cecal bleeding. A. Superior mesenteric artery angiogram showing contrast extravasation (arrow) in cecum. B. Superselective angiograms showing large amount of contrast extravasation (arrow) in cecum. C. 2 × 3 mm tornado microcoil (arrow) was placed in marginal artery with successful cessation of bleeding. D. Marked wall thickening of cecum (arrow) was noted on follow-up CT image 3 days after embolization. Abscess formation in pericecal (curved arrow) and subcutaneous region (arrow head) was also noted.
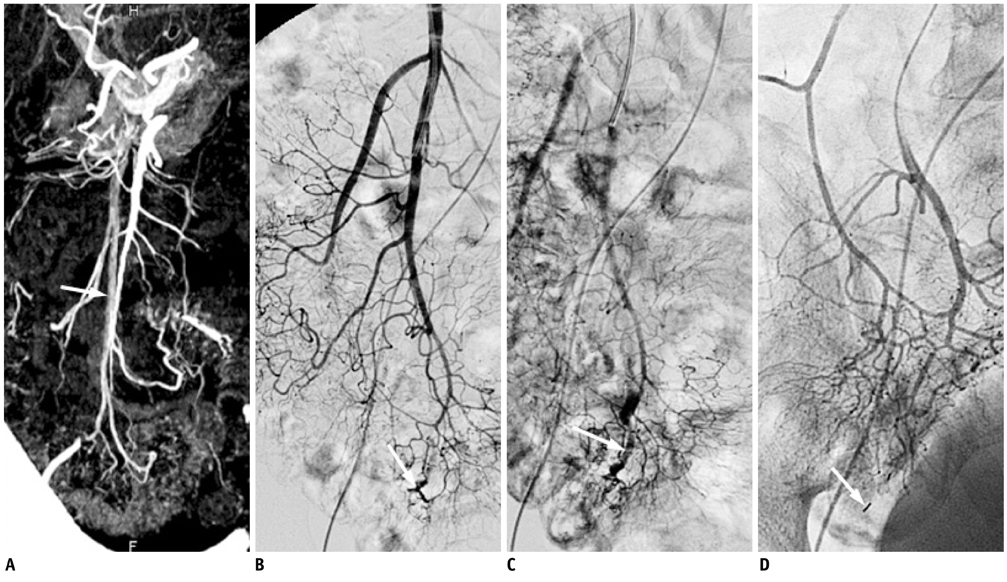
Fig. 4 72-year-old female with angiodysplasia. A. MDCT showing early opacification of right mesenteric veins (arrow) and segmental engorged submucosal vein (curved arrow) at distal ileum. No contrast extravasation on MDCT images can be identified. B. On superior mesenteric artery angiograms, no contrast extravasation can be identified but enlarged vascular tufts (arrow) in distal ileum are evident. C. Engorged submucosal vein (arrow) of distal ileum is also demonstrated in late arterial phase. D. After superselective microcoil embolization (arrow), follow-up angiograms showed disappearance of enlarged supplying artery and submucosal vein. MDCT = multidetector computed tomography
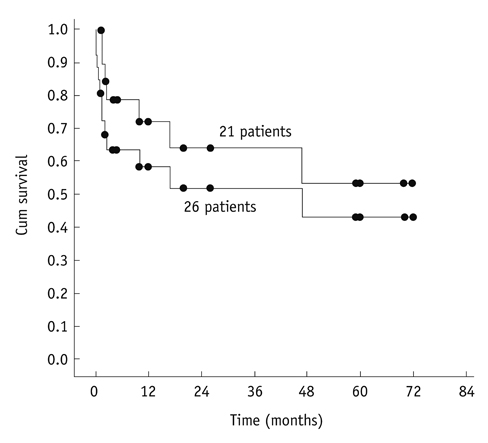
Fig. 5 Overall survival rates in twenty-six intended embolized patients and in twenty-one patients with survival for more than 30 days.
Reference
-
1. Longstreth GF. Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1997. 92:419–424.2. Koh DC, Luchtefeld MA, Kim DG, Knox MF, Fedeson BC, Vanerp JS, et al. Efficacy of transarterial embolization as definitive treatment in lower gastrointestinal bleeding. Colorectal Dis. 2009. 11:53–59.3. Billingham RP. The conundrum of lower gastrointestinal bleeding. Surg Clin North Am. 1997. 77:241–252.4. Peter DJ, Dougherty JM. Evaluation of the patient with gastrointestinal bleeding: an evidence based approach. Emerg Med Clin North Am. 1999. 17:239–261. x5. Gordon RL, Ahl KL, Kerlan RK, Wilson MW, LaBerge JM, Sandhu JS, et al. Selective arterial embolization for the control of lower gastrointestinal bleeding. Am J Surg. 1997. 174:24–28.6. Funaki B, Kostelic JK, Lorenz J, Ha TV, Yip DL, Rosenblum JD, et al. Superselective microcoil embolization of colonic hemorrhage. AJR Am J Roentgenol. 2001. 177:829–836.7. Bandi R, Shetty PC, Sharma RP, Burke TH, Burke MW, Kastan D. Superselective arterial embolization for the treatment of lower gastrointestinal hemorrhage. J Vasc Interv Radiol. 2001. 12:1399–1405.8. Sheth R, Someshwar V, Warawdekar G. Treatment of acute lower gastrointestinal hemorrhage by superselective transcatheter embolization. Indian J Gastroenterol. 2006. 25:290–294.9. Defreyne L, Vanlangenhove P, De Vos M, Pattyn P, Van Maele G, Decruyenaere J, et al. Embolization as a first approach with endoscopically unmanageable acute non variceal gastrointestinal hemorrhage. Radiology. 2001. 218:739–748.10. d'Othée BJ, Surapaneni P, Rabkin D, Nasser I, Clouse M. Microcoil embolization for acute lower gastrointestinal bleeding. Cardiovasc Intervent Radiol. 2006. 29:49–58.11. Maleux G, Roeflaer F, Heye S, Vandersmissen J, Vliegen AS, Demedts I, et al. Long-term outcome of transcatheter embolotherapy for acute lower gastrointestinal hemorrhage. Am J Gastroenterol. 2009. 104:2042–2046.12. Weldon DT, Burke SJ, Sun S, Mimura H, Golzarian J. Interventional management of lower gastrointestinal bleeding. Eur Radiol. 2008. 18:857–867.13. Loffroy R, Cercueil JP, Guiu B, Krausé D. Detection and localization of acute lower gastrointestinal bleeding prior to therapeutic endovascular embolization: a challenge! Am J Gastroenterol. 2009. 104:3108–3109. author reply 3109-3110.14. Lipof T, Sardella WV, Bartus CM, Johnson KH, Vignati PV, Cohen JL. The efficacy and durability of super-selective embolization in the treatment of lower gastrointestinal bleeding. Dis Colon Rectum. 2008. 51:301–305.15. Ahmed TM, Cowley JB, Robinson G, Hartley JE, Nicholson AA, Lim M, et al. Long term follow-up of transcatheter coil embolotherapy for major colonic haemorrhage. Colorectal Dis. 2010. 12:1013–1017.16. Drooz AT, Lewis CA, Allen TE, Citron SJ, Cole PE, Freeman NJ, et al. Quality improvement guidelines for percutaneous transcatheter embolization. J Vasc Interv Radiol. 2003. 14(9 Pt 2):S237–S242.17. Zuckerman GR, Prakash C. Acute lower intestinal bleeding: part I: clinical presentation and diagnosis. Gastrointest Endosc. 1998. 48:606–617.18. Kwak HS, Han YM, Lee ST. The clinical outcomes of transcatheter microcoil embolization in patients with active lower gastrointestinal bleeding in the small bowel. Korean J Radiol. 2009. 10:391–397.19. Leitman IM, Paull DE, Shires GT 3rd. Evaluation and management of massive lower gastrointestinal hemorrhage. Ann Surg. 1989. 209:175–180.20. Kuo WT, Lee DE, Saad WE, Patel N, Sahler LG, Waldman DL. Superselective microcoil embolization for the treatment of lower gastrointestinal hemorrhage. J Vasc Interv Radiol. 2003. 14:1503–1509.21. Khanna A, Ognibene SJ, Koniaris LG. Embolization as first-line therapy for diverticulosis-related massive lower gastrointestinal bleeding: evidence from a meta-analysis. J Gastrointest Surg. 2005. 9:343–352.22. Darcy M. Treatment of lower gastrointestinal bleeding: vasopressin infusion versus embolization. J Vasc Interv Radiol. 2003. 14:535–543.23. Browder W, Cerise EJ, Litwin MS. Impact of emergency angiography in massive lower gastrointestinal bleeding. Ann Surg. 1986. 204:530–536.24. Sherman LM, Shenoy SS, Cerra FB. Selective intra-arterial vasopressin: clinical efficacy and complications. Ann Surg. 1979. 189:298–302.25. Bookstein JJ, Chlosta EM, Foley D, Walter JF. Transcatheter hemostasis of gastrointestinal bleeding using modified autogenous clot. Radiology. 1974. 113:277–285.26. Chuang VP, Wallace S, Zornoza J, Davis LJ. Transcatheter arterial occlusion in the management of rectosigmoidal bleeding. Radiology. 1979. 133(3 Pt 1):605–609.27. Rosenkrantz H, Bookstein JJ, Rosen RJ, Goff WB 2nd, Healy JF. Postembolic colonic infarction. Radiology. 1982. 142:47–51.28. Luchtefeld MA, Senagore AJ, Szomstein M, Fedeson B, Van Erp J, Rupp S. Evaluation of transarterial embolization for lower gastrointestinal bleeding. Dis Colon Rectum. 2000. 43:532–534.29. Kickuth R, Rattunde H, Gschossmann J, Inderbitzin D, Ludwig K, Triller J. Acute lower gastrointestinal hemorrhage: minimally invasive management with microcatheter embolization. J Vasc Interv Radiol. 2008. 19:1289–1296.e2.30. Pennoyer WP, Vignati PV, Cohen JL. Management of angiogram positive lower gastrointestinal hemorrhage: long term follow-up of non-operative treatments. Int J Colorectal Dis. 1996. 11:279–282.31. Weldon DT, Burke SJ, Sun S, Mimura H, Golzarian J. Interventional management of lower gastrointestinal bleeding. Eur Radiol. 2008. 18:857–867.32. Nicholson AA, Ettles DF, Hartley JE, Curzon I, Lee PW, Duthie GS, et al. Transcatheter coil embolotherapy: a safe and effective option for major colonic haemorrhage. Gut. 1998. 43:79–84.33. Peck DJ, McLoughlin RF, Hughson MN, Rankin RN. Percutaneous embolotherapy of lower gastrointestinal hemorrhage. J Vasc Interv Radiol. 1998. 9:747–751.34. Cynamon J, Atar E, Steiner A, Hoppenfeld BM, Jagust MB, Rosado M, et al. Catheter-induced vasospasm in the treatment of acute lower gastrointestinal bleeding. J Vasc Interv Radiol. 2003. 14(2 Pt 1):211–216.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Update of Embolization of Upper Gastrointestinal Tract Bleeding
- The Effect of Embolotherapy for Acute Gastrointestinal Bleeding in Patient with Coagulopathy
- Superselective Embolization with Microcoil in Acute Gastrointestinal Hemorrhage
- The Clinical Outcomes of Transcatheter Microcoil Embolization in Patients with Active Lower Gastrointestinal Bleeding in the Small Bowel
- Three Cases of Gastrointestinal Bleeding Controlled by Temporary Occlusion using Balloon Catheter
