Volar Percutaneous Cannulated Screw Fixation for Subacute Scaphoid Wasit Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, School of Medicine, Ewha Womans University, Seoul, Korea. kimjk@ewha.ac.kr
- KMID: 1470023
- DOI: http://doi.org/10.12671/jkfs.2009.22.2.104
Abstract
-
PURPOSE: To report the surgical results of volar percutaneous cannulated compression screw fixation in subacute scaphoid fracture.
MATERIALS AND METHODS
Between January 2004 and January 2007, eight consecutive patients with subacute scaphoid waist fracture, who sought medical attention between 4 weeks to 6 months after injury, were included in this study. All patients were male of an average age 29.2 years (range, 19 to 44). Mean duration of injury was 10.3+/-4.1 weeks. An acutrak cannulated screw (Acumed, Hillsboro, OR) was introduced volarly under image intensifier guidance in all patients. We performed radiological evaluation preoperatively and postoperatively. And we performed 12 months postoperatively using grip strength, range of motion (ROM) of the wrist, Mayo Modified Wrist Score (MMWS) and Disabilities of the Arm, Shoulder and the Hand (DASH) score for functional evaluation.
RESULTS
Preoperative radiography showed minimal sclerosis line in three patients and a bone resorption around fracture sites in two patients. However, no patient had dorsal intercalated segment instability or more than 35 degrees of lateral intrascaphoid angle. Fractures united successfully at 11.6+/-2.1 weeks postoperatively without any requirement for a further procedure. At 12 months follow-up evaluations, ROM of the injured wrist was 93% of the uninjured wrist and grip strength of the injured wrist was 95% of the injured wrist. The mean MMWS was 93+/-6.6 and the mean DASH score was 4.8+/-1.2.
CONCLUSION
We believe that volar percutaneous cannulated screw fixation is a reliable method in case of subacute scaphoid waist fracture without scaphoid deformity or carpal instability.
MeSH Terms
Figure
-
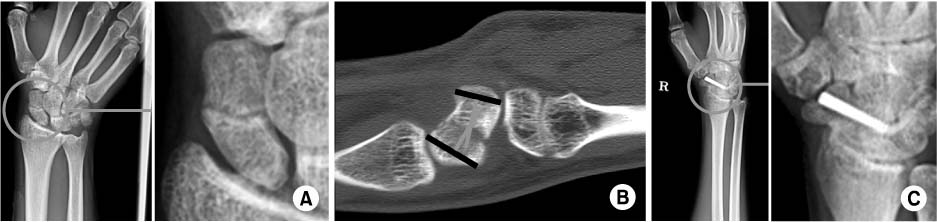
Fig. 1 Subacute scaphoid waist fracture with minimal sclerosis. (A) Anteroposterior radiograph shows a minimal sclerotic line around the fracture. (B) Lateral intrascaphoid angle is 28 degrees in CT. (C) Healing was achieved 10 weeks after volar percutaenous screw insertion.
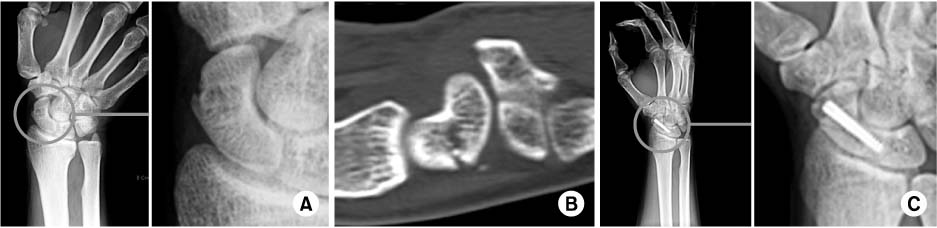
Fig. 2 Subacute scaphoid waist fracture with cyst formation. (A) Anteroposterior radiograph shows cyst formation with bone resorption at the fracture. (B) CT shows cyst formation with bone resorption at the waist of scaphoid. (C) Healing was achieved 14 weeks after volar percutaenous screw insertion.
Cited by 1 articles
-
Surgical Outcome of Stable Scaphoid Nonunion without Bone Graft
Eun Sun Moon, Myung Sun Kim, Il Kyu Kong, Min Sun Choi
J Korean Fract Soc. 2010;23(1):69-75. doi: 10.12671/jkfs.2010.23.1.69.
Reference
-
1. Adamany DC, Mikola EA, Fraser BJ. Percutaneous fixation of the scaphoid through a dorsal approach: an anatomic study. J Hand Surg Am. 2008; 33:327–331.
Article2. Adolfsson L, Lindau T, Arner M. Acutrak screw fixation versus cast immobilisation for undisplaced scaphoid waist fractures. J Hand Surg Br. 2001; 26:192–195.
Article3. Anderson M, Larson A, Moran S, Cooney W, Amrami K, Berger R. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am. 2008; 33:675–682.
Article4. Bond C, Shin A, McBride M, Dao K. Percutaneous screw fixation or cast immobilization for nondisplaced scaphoid fractures. J Bone Joint Surg Am. 2001; 83:483–488.
Article5. Chan KW, McAdams TR. Central screw placement in percutaneous screw scaphoid fixation: a cadaveric comparison of proximal and distal techniques. J Hand Surg Am. 2004; 29:74–97.
Article6. Cooney WP, Linscheid RL, Dobyns JH. Triangular fibrocartilage tears. J Hand Surg Am. 1994; 19:143–154.
Article7. Eddeland A, Eiken O, Hellgren E, Ohlsson NM. Fractures of the scaphoid. Scand J Plast Reconstr Surg. 1975; 9:234–239.
Article8. Gasser H. Delayed union and pseudarthrosis of the carpal navicular: treatment by compression-screw osteosynthesis; a preliminary report on twenty fractures. J Bone Joint Surg Am. 1965; 47:249–266.9. Gupta A, Risitano G, Crawford RJ, Burke FD. The Ununited Scaphoid: prognostic factors in delayed and nonunions of the scaphoid. Hand Surg. 1999; 4:11–19.
Article10. Herbert T, Fisher W. Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br. 1984; 66:114–123.
Article11. Kang ES, Kang HJ, Lee KS. Open reduction & internal fixation for the nonunion of scaphoid fracture. J Korean Soc Fract. 1996; 9:8–14.
Article12. Korkala O, Antti-Poika I. Late treatment of scaphoid fractures by bone grafting and compression staple osteosynthesis. J Hand Surg Am. 1989; 14:491–495.
Article13. Oka K, Moritomo H, Murase T, Goto A, Sugamoto K, Yoshikawa H. Patterns of bone defect in scaphoid nonunion: a 3-dimensional and quantitative analysis. J Hand Surg Am. 2005; 30:359–365.
Article14. Langhoff O, Andersen JL. Consequences of late immobilization of scaphoid fractures. J Hand Surg Br. 1988; 13:77–79.
Article15. Lee JY, Lim JY, Oh JH, Ko YM. Cross-cultural adaptation and clinical evaluation of a Korean version of the disabilities of arm, shoulder and hand outcome questionnaire (K-DASH). J Shoulder Elbow Surg. 2008; 17:570–574.
Article16. Leyshon A, Ireland J, Trickey E. The treatment of delayed union and non-union of the carpal scaphoid by screw fixation. J Bone Joint Surg Br. 1984; 66:124–127.
Article17. Little C, Burston B, Hopkinson-Woolley J, Burge P. Failure of surgery for scaphoid non-union is associated with smoking. J Hand Surg Br. 2006; 31:252–255.
Article18. Mack GR, Wilckens JH, McPherson SA. Subacute scaphoid fractures. A closer look at closed treatment. Am J Sports Med. 1998; 26:56–58.19. Moritomo H, Viegas SF, Elder KW, et al. Scaphoid nonunion: a 3-dimensional analysis of patterns of deformity. J Hand Surg Am. 2000; 25:520–528.20. Shin JI, Kim TS, Lee SJ. Surgical treatment of scaphoid nonunion. J Korean Soc Fract. 1996; 9:15–23.
Article21. Simonian PT, Trumble TE. Scaphoid nonunion. J Am Acad Orthop Surg. 1994; 2:185–191.
Article22. Slade JF 3rd, Dodds SD. Minimally invasive management of scaphoid nonunions. Clin Orthop Relat Res. 2006; 445:108–119.
Article23. Slade JF 3rd, Geissler WB, Gutow AP, Merrell GA. Percutaneous internal fixation of selected scaphoid nonunions with an arthroscopically assisted dorsal approach. J Bone Joint Surg Am. 2003; 85:Suppl 4. 20–32.
Article24. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid. Treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am. 1996; 78:1829–1837.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Computed Tomographic Analysis of Screw Positions in Volar Percutaneous Screw Fixation of Scaphoid Fractures
- Modified Volar Percutaneous Screw Fixation for the Scaphoid Fractures: Trans-trapezial Approach
- The Treatment of Volar Iunate Dislocation and Perilunar Dislocation
- Arthroscopy Assisted Percutaneous Reduction and Screw Fixation of a Displaced Intra-articular Glenoid Fracture: A Case Report
- Percutaneous Cannulated Screw Fixation of Fifth Proximal Metatarsal Stress Fracture in Athletes
