Colon Type Adenocarcinoma of Appendiceal Orifice with Synchronous Colon Cancer and Appendiceal Mucocele
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Cheju National University, Jeju, Korea.
- 2Department of Surgery, School of Medicine, Cheju National University, Jeju, Korea. 41056@naver.com
- 3Department of Pathology, School of Medicine, Cheju National University, Jeju, Korea.
- 4Department of Surgery, School of Medicine, Ajou University, Suwon, Korea.
- 5Department of Pathology, College of Medicine, Seoul National University, Seoul, Korea.
- KMID: 1464958
- DOI: http://doi.org/10.4174/jkss.2009.76.6.398
Abstract
- Primary adenocarcinoma of the appendix is an extraordinarily rare tumor, with fewer than 500 cases described in the collected world literature. However, it has been shown that the incidence of secondary neoplasm, such as synchronous or metachronous lesions, for primary adenocarcinoma of the appendix is much greater than that for colorectal cancer in general. In the present paper, the authors report a case of a 72-year-old male patient with immunoreactivity for P 53 and DCC protein and a review of the literature, who was operated on for an appendiceal orifice cancer and in whom colonic adenomas, a synchronous colon cancer and an appendiceal mucocele, was incidentally discovered after right hemicolectomy.
MeSH Terms
Figure
-
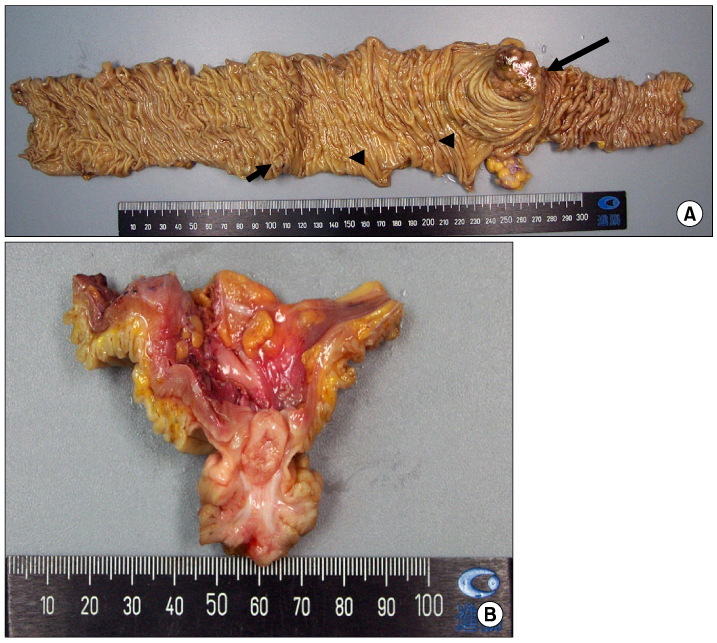
Fig. 1 The specimen. (A) The length of resected colon and cecum is 23 cm and 6 cm, respectively. About 4×3×3 cm sized round polypoid mass is seen on the cecal base (long arrow). About 1.5×0.7×0.5 cm sized ulcerated mass is noticed on the ascending colon (short arrow). Additional small polyps are seen between 1st and 2nd masses (arrow heads). (B) On transverse section of appendix, mass originates from appendix orifice and has short stalk-like structure.
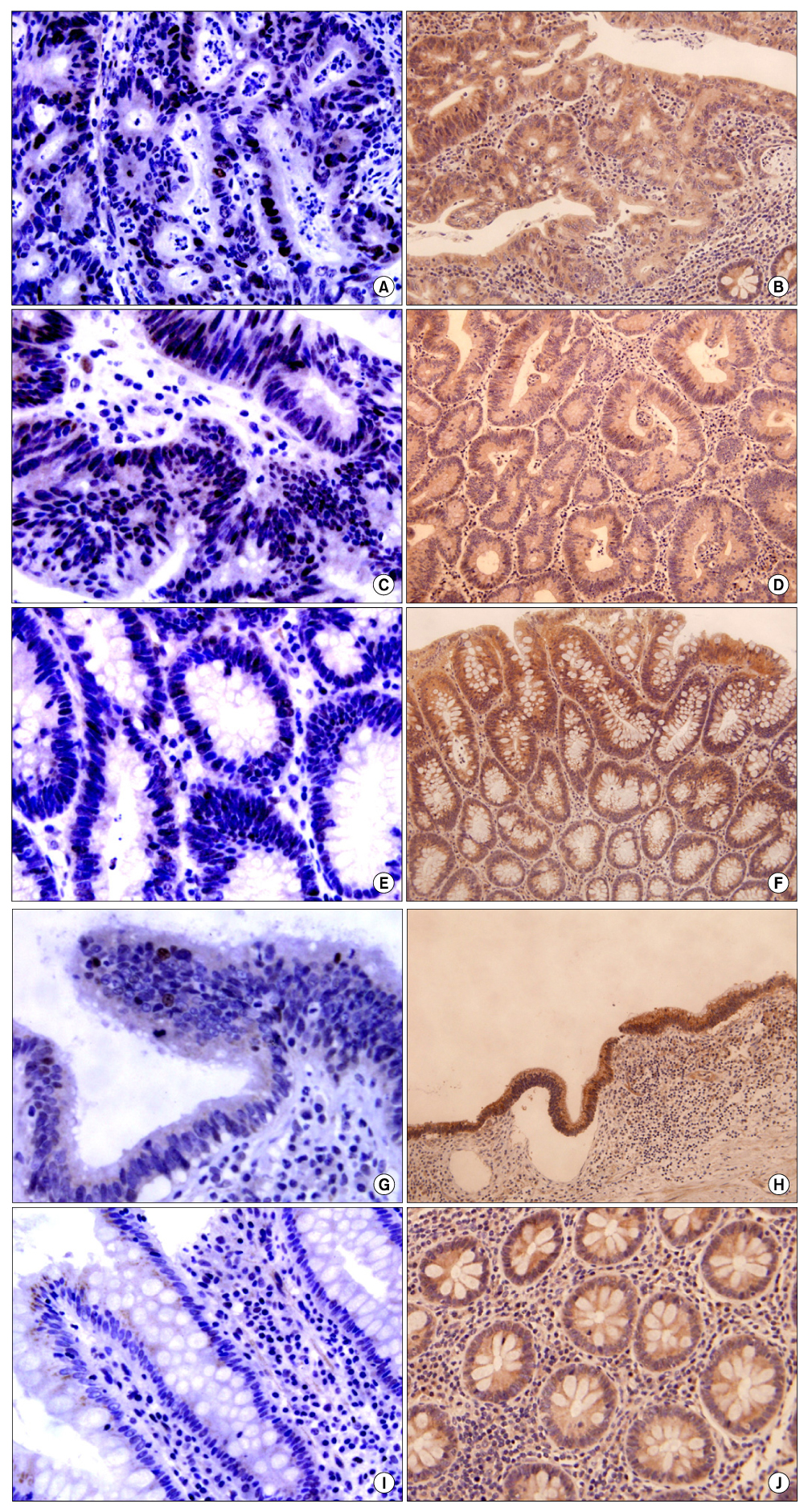
Fig. 2 Immunohistochemical analysis of the expression of DCC (A, C, E, G and I, ×400) and p53 (B, D, F, H and J, ×200) in appendiceal and colonic adenocarcinoma (A~C and D), adenoma (E and F), appendiceal mucocele (G and H) and normal colonic mucosa (I and J). DCC protein was expressed uniformly in normal colonic crypts and luminal cells with cytoplasmic pattern (I). DCC protein was also expressed in neoplastic lesion including adenocarcinoma (A and C), adenoma (E), and mucocele (G) with more intense staining than normal mucosa (J). P53 over-expression is seen in adenocarcinoma (in more than 75% of tumor cells) (B and D) and adenoma (in 25~50% of tumor cells) (F) contrast to no staining of normal colonic mucosa (J). In mucocele of appendix, a few epithelial cells stained with p53 (G).
Reference
-
1. Connor SJ, Hanna GB, Frizelle FA. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum. 1998. 41:75–80.2. Nitecki SS, Wolff BG, Schlinkert R, Sarr MG. The natural history of surgically treated primary adenocarcinoma of the appendix. Ann Surg. 1994. 219:51–57.3. Ferro M, Anthony PP. Adenocarcinoma of the appendix. Dis Colon Rectum. 1985. 28:457–459.4. Cho JB, Cho HJ, Shin OR, Kim KH, Ahn CH, Kim JS, et al. Clinical findings of appendiceal mucocele. J Korean Surg Soc. 2008. 74:429–435.5. Deans GT, Spence RA. Neoplastic lesions of the appendix. Br J Surg. 1995. 82:299–306.6. Younes M, Katikaneni PR, Lechago J. Association between mucosal hyperplasia of the appendix and adenocarcinoma of the colon. Histopathology. 1995. 26:33–37.7. Kataoka M, Okabayashi T, Johira H, Nakatani S, Nakashima A, Takeda A, et al. Aberration of p53 and DCC in gastric and colorectal cancer. Oncol Rep. 2000. 7:99–103.8. Shibata D, Reale MA, Lavin P, Silverman M, Fearon ER, Steele G Jr, et al. The DCC protein and prognosis in colorectal cancer. N Engl J Med. 1996. 335:1727–1732.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Appendiceal Mucocele with Concominant Colon Cancer
- Mucocele of the Appendix Secondary to Obstruction by Cecal Endometriosis
- A Case of Appendiceal Mucocele
- Appendiceal Mucocele in a Patient with Normal Colonoscopic Findings
- Appendiceal Mucocele Developed by Appendiceal Mucosal Prolapse: A Rare Case Report with Review of Literature
