Surgical Outcome of Stable Scaphoid Nonunion without Bone Graft
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonnam National University School of Medicine, Gwangju, Korea. kongilkyu@gmail.com
- KMID: 1461575
- DOI: http://doi.org/10.12671/jkfs.2010.23.1.69
Abstract
- PURPOSE
To evaluate the results of Acutrak-screw fixation without bone-graft for the treatment of stable scaphoid nonunion and to assess its prognostic factors.
MATERIALS AND METHODS
Fifteen patients who underwent internal fixation using Acutrak-screw without bone graft for stable scaphoid nonunion were studied. Standard radiographs and CT were analyzed for degenerative changes (presence of cystic change and periscaphoid osteoarthritis), the nonunion site using fragment ratio and union. Clinically, patients age and the interval to surgery were evaluated.
RESULTS
Mean follow-up duration was 31 months and 11 of 15 (73.3 percentages) cases healed at mean time of 12.8 weeks. Fragment ratio of nonunion site was 37.2 percentages in nonunion group and 54.2 percentages in union group (p=0.016). Presence of cystic change and periscaphoid osteoarthritis showed no singnificant statistical difference in both groups. Younger age lower than 20 years was closely related with bone union (p=0.001). But there were little correlation between bone union and interval to surgery.
CONCLUSION
Internal fixation without bone graft showed 73.3 percentages of overall union rate in the treatment of stable scaphoid nonunion. And young patients who have distally located stable scaphoid nonunion can be successfully treated with internal fixation without bone graft.
Keyword
Figure
-
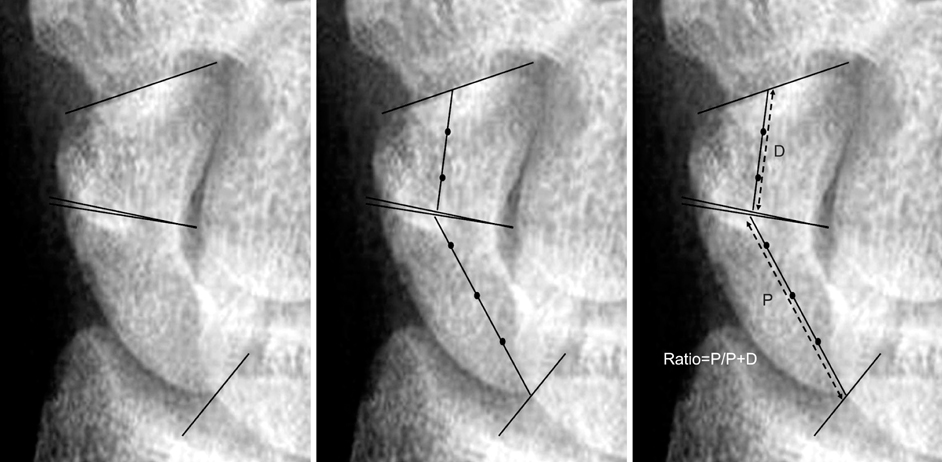
Fig. 1 Fragment ratio. Horizontal lines were drawn to define the extent of the fragment. The middle of the fragment was identified and a midline was drawn connecting the two horizontal lines. The lengths of these lines (P, D) were measured to determine the fragment size (P: Proximal fragment, D: Distal fragment).

Fig. 2 (A) Radiographs of 22 years old male shows slightly proximally located nonunion of scaphoid. (B) Serial follow-up radiographs and (C) computer tomography at postoperative 8 month show failure of healing process.

Fig. 3 (A) Radiographs of 47 years old male shows proximally located nonunion of scaphoid. (B) Computer tomography demonstrates cystic change of nonunion site and degenerative change of radial styloid and radioscaphoid joint. (C) Serial follow-up radiographs show failure of healing process at 4 months postoperatively.

Fig. 4 (A) Radiographs of 16 years old female shows suspicious finding of distally located nonunion of scaphoid. (B) Computer tomography demonstrates cystic change of nonunion site. (C) Serial follow-up radiographs show complete union at about 12 weeks after surgery.
Reference
-
1. Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP 3rd, Linscheid RL. Scaphoid malunion. J Hand Surg Am. 1989. 14:679–687.
Article2. Amadio PC, Moran SL. Green DP, editor. Fractures of the carpal bone. Operative hand surgery. 2005. 5th ed. Philadelphia: Churchill Livingstone;711–779.3. Amadio PC, Taleisnik J. Green DP, editor. Fractures of the carpal bone. Operative hand surgery. 1993. 3rd ed. New York: Churchill Livingstone;799–860.4. Chloros GD, Themistocleous GS, Wiesler ER, Benetos IS, Efstathopoulos DG, Soucacos PN. Pediatric scaphoid nonunion. J Hand Surg Am. 2007. 32:172–176.
Article5. Cosio MQ, Camp RA. Percutaneous pinning of symptomatic scaphoid nonunions. J Hand Surg Am. 1986. 11:350–355.
Article6. Dias JJ. Definition of union after acute fracture and surgery for fracture nonunion of the scaphoid. J Hand Surg Br. 2001. 26:321–325.
Article7. Dodds SD. Minimally invasive management of scaphoid nonunions. Clin Orthop Relat Res. 2006. 445:108–119.
Article8. Ikeda K, Osamura N, Tomita K. Percutaneous screw fixation without bone graft for cystic-type scaphoid fractures. J Trauma. 2008. 65:1453–1458.
Article9. Jeon IH, Kochhar H, Lee BW, Kim SY, Kim PT. Percutaneous screw fixation for scaphoid nonunion in skeletally immature patients: a report of two cases. J Hand Surg Am. 2008. 33:656–659.
Article10. Kim JK, Kim JO, Lee SY, Do NH. Volar percutaneous cannulated screw fixation for subacute scaphoid wasit fracture. J Korean Fract Soc. 2009. 22:104–109.
Article11. Merrell G, Slade J. Technique for percutaneous fixation of displaced and nondisplaced acute scaphoid fractures and select nonunions. J Hand Surg Am. 2008. 33:966–973.
Article12. Merrell GA, Wolfe SW, Slade JF 3rd. Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am. 2002. 27:685–691.
Article13. Ramamurthy C, Cutler L, Nuttall D, Simison AJ, Trail IA, Stanley JK. The factors affecting outcome after non-vascular bone grafting and internal fixation for nonunion of the scaphoid. J Bone Joint Surg Br. 2007. 89:627–632.
Article14. Schneider LH, Aulicino P. Nonunion of the carpal scaphoid: the Russe procedure. J Trauma. 1982. 22:315–319.15. Schuind F, Haentjens P, Van Innis F, Vander Maren C, Garcia-Elias M, Sennwald G. Prognostic factors in the treatment of carpal scaphoid nonunions. J Hand Surg Am. 1999. 24:761–776.
Article16. Shah J, Jones WA. Factors affecting the outcome in 50 cases of scaphoid nonunion treated with Herbert screw fixation. J Hand Surg Br. 1998. 23:680–685.
Article17. Shim JI, Kim TS, Lee SJ, Lee SH, Yoo CM, Han KJ. Surgical treatment of scaphoid nonunion. J Korean Soc Fract. 1996. 9:15–23.
Article18. Slade JF 3rd, Geissler WB, Gutow AP, Merrell GA. Percutaneous internal fixation of selected scaphoid nonunions with an arthroscopically assisted dorsal approach. J Bone Joint Surg Am. 2003. 85:Suppl 4. 20–32.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Bone Grafting and Kirschner-Wires Fixation for Scaphoid Nonunion
- The Effect of Smoking on the Outcomes of Vascularized Bone Graft Surgery in Scaphoid Nonunion through Meta-analysis
- Arthroscopic Bone Grafting and Percutaneous K-Wires Fixation for the Treatment of Scaphoid Nonunion: Surgical Technique
- Treatment of Scaphoid Fractures and Nonunions
- Scaphoid Fractures and Nonunion
