Classification of microvascular anastomosis in oral and maxillofacial reconstruction
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Dental research institute, School of Dentistry, Seoul National University, Seoul, Korea. smin5@snu.ac.kr
- KMID: 1449064
- DOI: http://doi.org/10.5125/jkaoms.2011.37.4.312
Abstract
- A reconstruction following a resection of malignant oral cavity tumors is one of the most difficult problems in recent oral oncology. For a better understanding of oral and maxillofacial reconstructive procedures, basic and advanced microvascular anastomosis techniques must be learned and memorized. The aim of this article was to clarify and define the microvascular anastomosis methods, such as primary closure after an arteriotomy, end to side anastomosis, end to end anastomosis, and side to side anastomosis with an artery and vein. This review article discusses the basic skills regarding microvascular anastomoses with brief schematic diagrams in the Korean language. This article is expected to be helpful, particularly to young doctors in the course of the Korean national board curriculum periods for oral and maxillofacial surgery.
Keyword
MeSH Terms
Figure
-
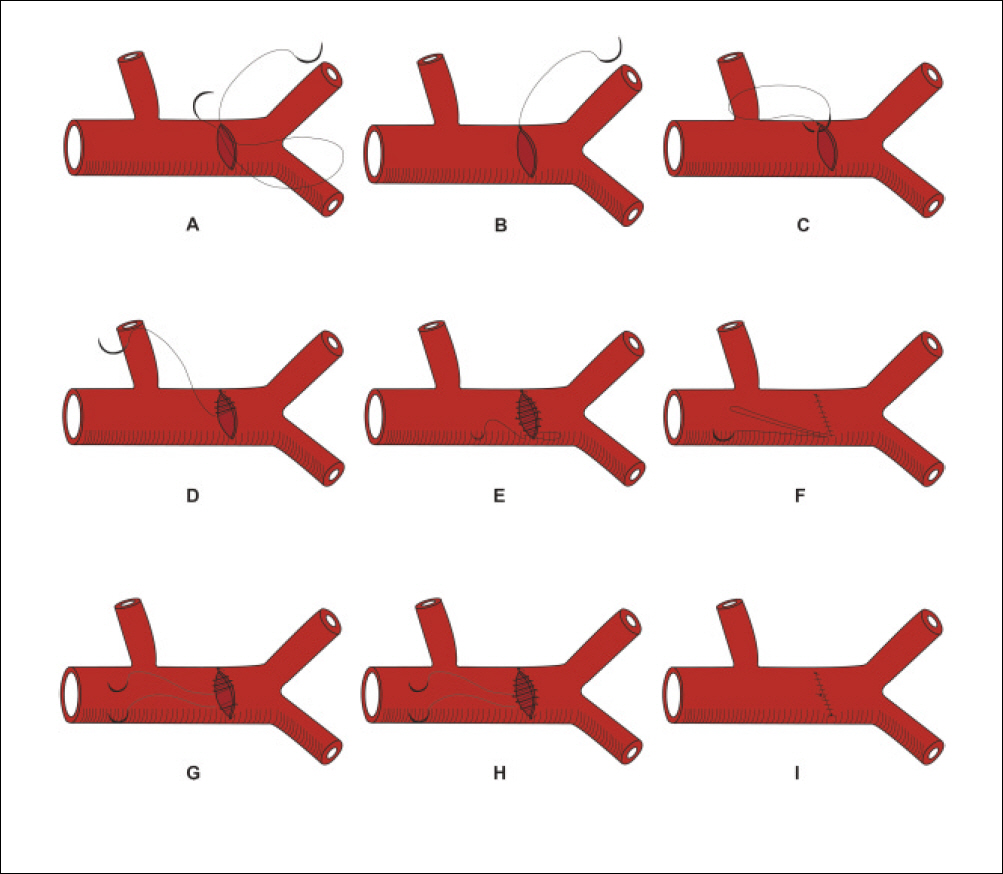
Fig. 1. Schematic drawings of primary continuous closure in the transverse arteriotomy. A. Introduce the needle from the intimal side of the arterial wall, B. Tie the suture and cut one end, C. Start running the suture towards the midpoint of the arteriotomy, D. Continuation of running the suture all the way towards the end of the arteriotomy, E. Place the last two bites closely spaced, F. Pull the suture and tie it to itself, G. Another alternate way of suture at the other end of the arteriotomy to avoid the need to tie the suture to itself, H. Run the second suture towards the midpoint of the arteriotomy, I. Tie both sutures.
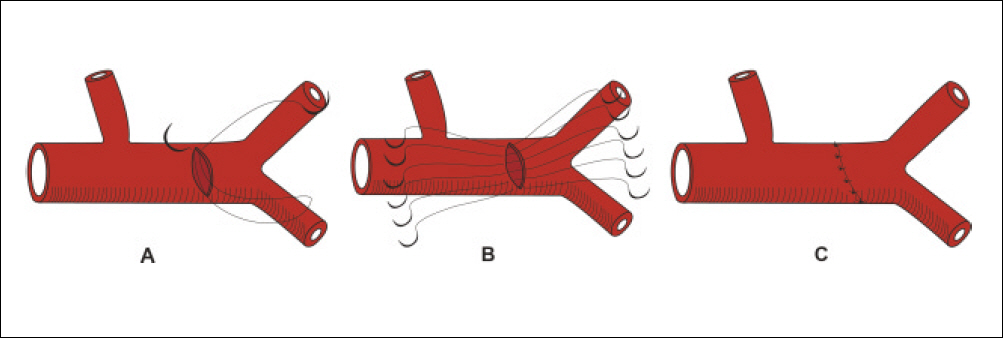
Fig. 2. Schematic drawings of primary interrupted closure in the tranverse arteriortomy. A. Introduce the needle from the intimal side of the arterial wall to avoid dissection of the plague, B. Place all the needles and sutures under direct vision, C. Pull and tie the sutures.
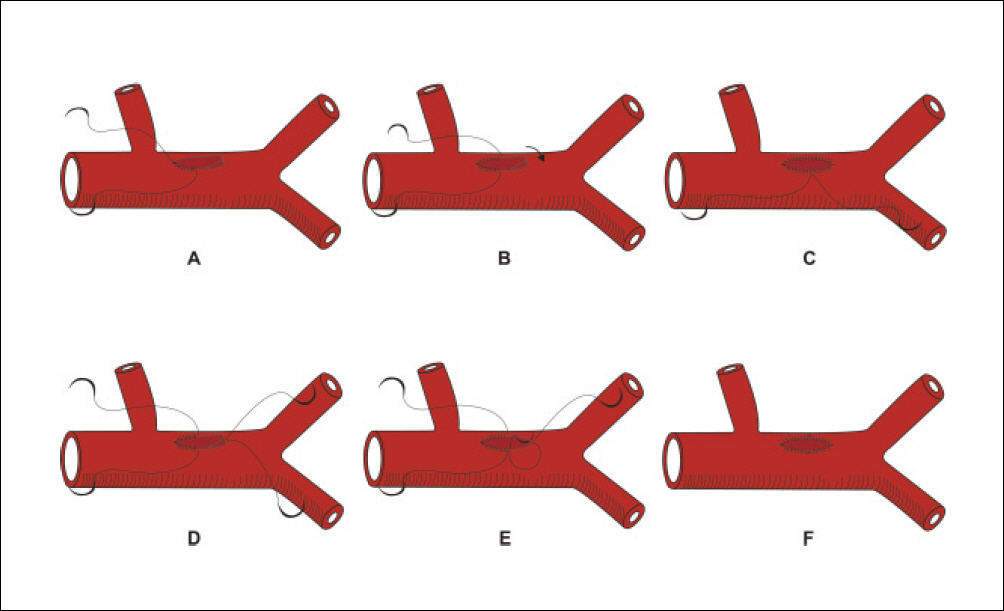
Fig. 3. Schematic drawings of Patch closure with anchor technique in the longitudinal arteriotomy. A. Run the suture to the midpoint of the arteriotomy, B. Similarly run the other end of the suture to the midpoint of the arteriotomy, C. Continuous running this suture until you reach the other end, D. Alternate starting another suture at the opposite end, after suturing one half of the patch, E. This suture may be a simple or a horizontal mattress suture, F. Tie both sutures.
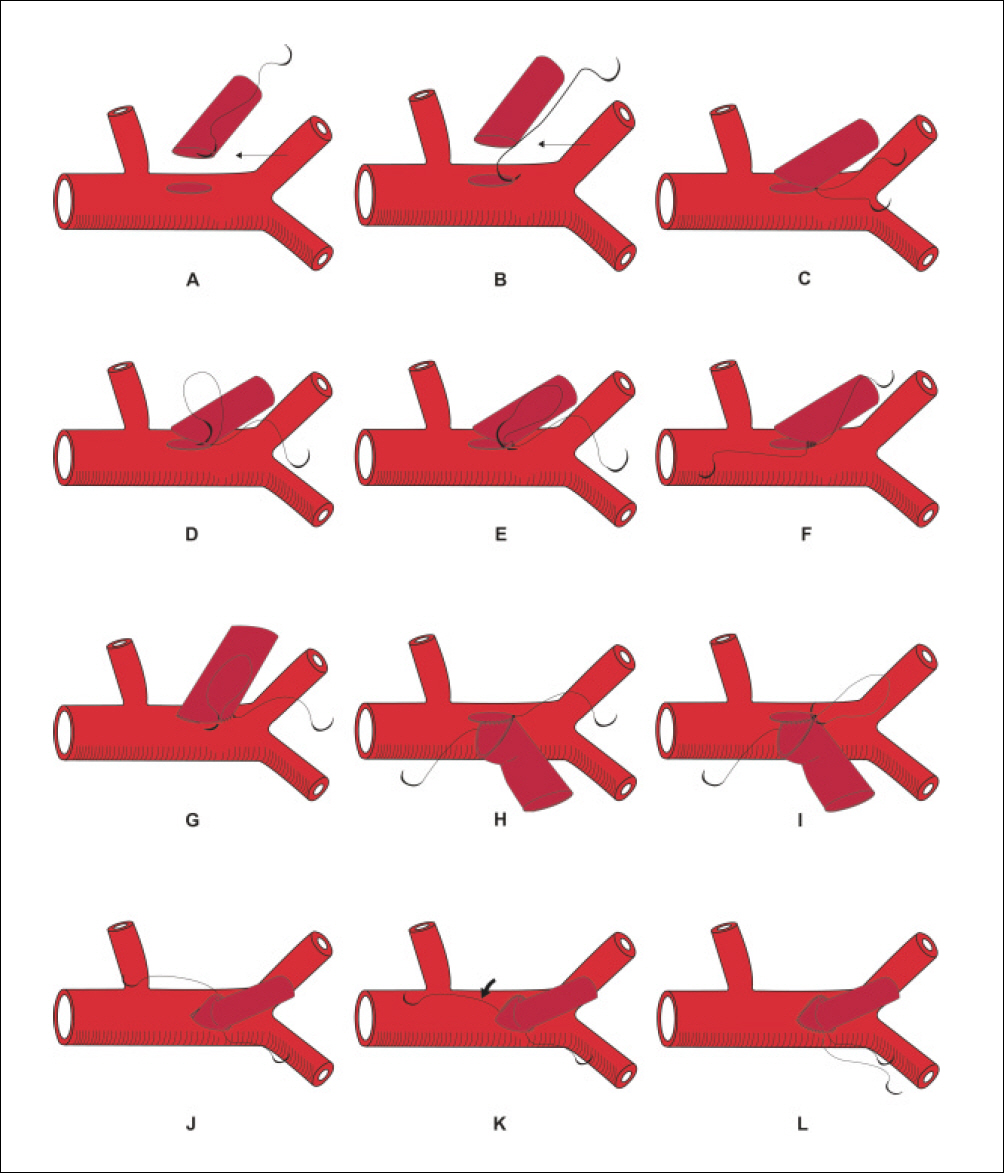
Fig. 4. Schematic drawings of simple anchoring sutures in the end-to-side anastomosis. A. Start at the center of the heel by introducing the needle outside to inside in the graft, B. Introduce the needle in a matching location from inside to outside. This suture may be a horizontal mattress suture or simple suture as shown here, C. Tie the suture, D. Continue with one end of the suture, E. Introduce the needle in the vessel with the first few bites after tying down the suture, F. Place several sutures on one side, G. Tighten the sutures with confirmation the graft and the artery together in a single bite, H. Place several bites, I. Start suturing on this side, J. Place several bites, K. Continuation with the upper suture and run it around the apex, L. Tie both sutures.
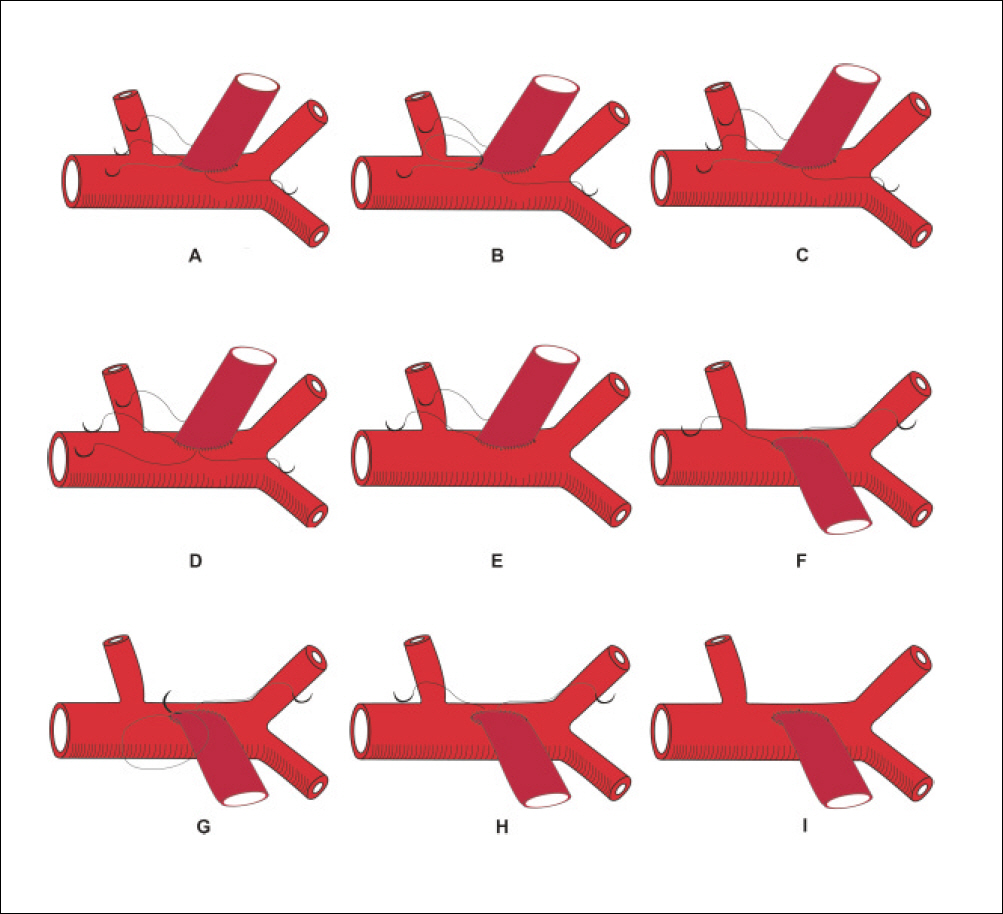
Fig. 5. Schematic drawings of alternate simple anchoring sutures in the end-to-side anastomosis. A. Starting a new suture at the apex, B. Tie the suture, C. Place several more bites, D. Run the suture line toward the heel until it meets the other suture, E. Tie both sutures together, F. Flip the graft to the other side, G. Introduce the needle from the adventitial side of the graft and the intimal side of the artery, H. Place several more bites, I. Tie the sutures.

Fig. 6. Schematic drawings of horizontal mattress anchoring sutures in the end-to-side anastomosis. A. The fixing sutures are horizontal mattress sutures, B. These mattress sutures may help fold the graft and the artery to achieve an everted suture line with an ideal intima-to-intima opposition, C. In small vessels, it is important to avoid taking wide horizontal mattress sutures at the toe or the heel, as they may cause puckering or narrowing of the lumen.
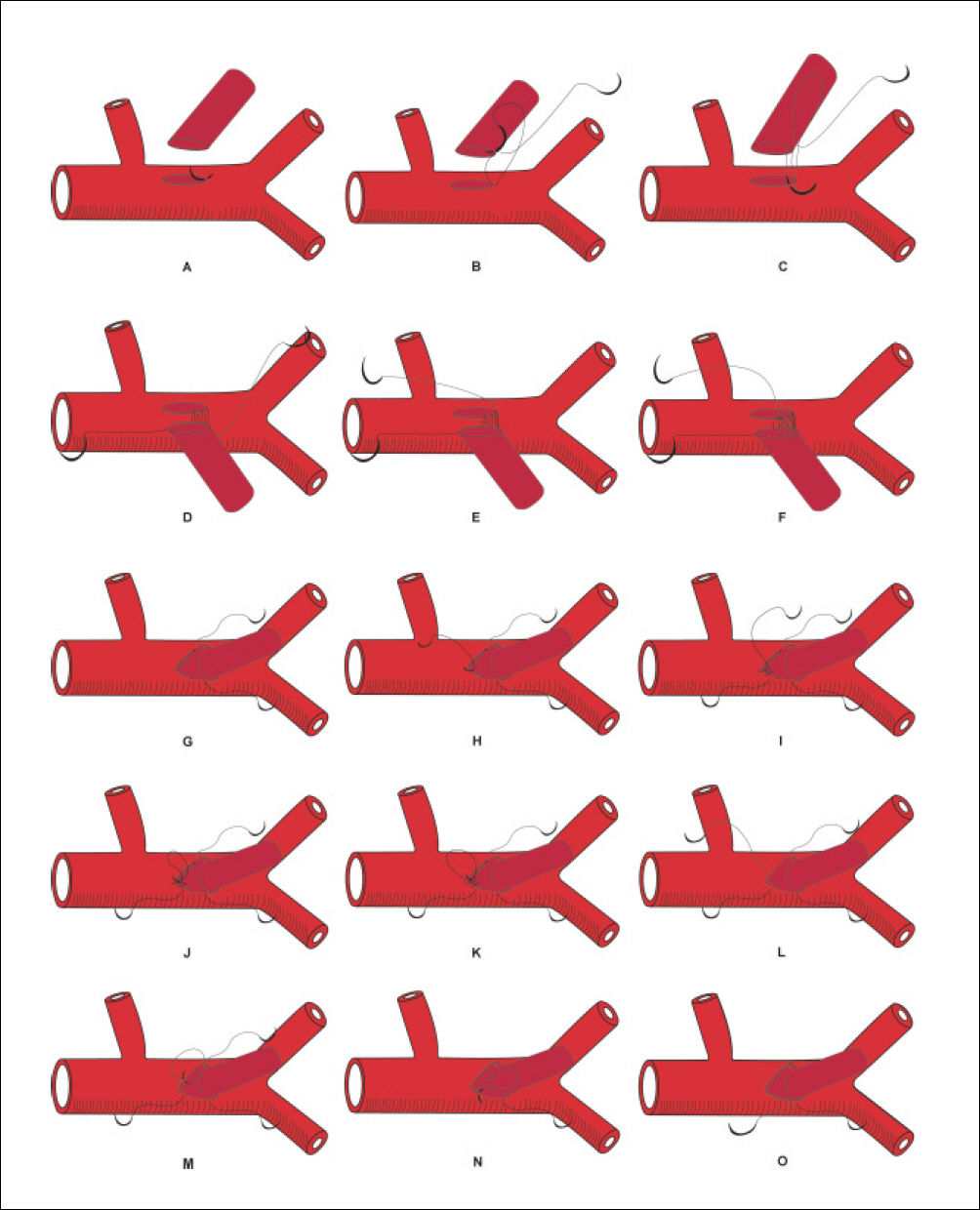
Fig. 7. Schematic drawings of anchorring sutures in the end-to-end anastomosis. A. Start by placing one suture at the base of each vessel, B. Tie the suture, C. Place an identical suture diametrically opposite to the first suture, D. Start suturing on the anterior wall, E. Run the suture along the anterior wall until it meets the inferior suture, F. Tie the sutures, G-I. Flip the graft 180�, bringing the posterior wall to an anterior location, J. Run the remaining end of the superior suture toward the inferior suture, K. Continuation with the superior suture until its meets the inferior suture, L. Alternate suturing with the lower suture toward the upper suture, M. This variation will avoid the need to tie to a suture that already has a knot at tis base, which could result in a bulky knot, N. Tie the sutures, O. Flip the graft back its original position.

Fig. 8. Schematic drawings of parachute sutures in the end-to-end anastomosis. A. Start the suture or continue suturing the back wall without tying, B. Introduce the needle from the adventitial side of‘A'vessel to the intimal side of ‘B'vessel, C. Allow the suturing to be performed in a forehand manner, D. Continue placing the sutures until the posterior suture line is completed, E. Tight the suture line, F. Continuation with the upper suture until it meets the other end with avoiding excessive tension on the suture line, G. A waist or purse string effect can occur at the anastomosis of excessive tension is applied to the suture line, H. Alternate start another simple mattress suture, I. Tie the suture and continue running the suture line, J. Alternate suturing without tying, K. Introduce the needle on the adventitial side of‘B'vessel and on the intimal side of ‘A’ vessel, L. Continue suturing until meet the inferior suture, M. Tie the sutures, N. Start suturing toward the superior suture, O. Tie the sutures.

Fig. 9. Schematic drawings of anchor techniques in the side-to-side anastomosis. A. Start by placing one suture at the midpoint of the venotomy from outside to inside, B. Introduce the needle in a corresponding point in the arteriotomy from inside to outside, C. Tie down the suture, D. The needle is introduce from the adventitial side of the vein and the intimal side of the artery, E. Continue suturing the back wall on one side of the suture, F. Complete the back wall on the other side of the suture in a similar manner, G. Resume suturing along the anterior wall. Introduce the needle inside-outside in the artery, H. Continue running the suture toward the lower suture, I. Tie the suture.
Reference
-
1. Yasagil MG. Reconstructive and constructive surgery of the cerebrovascular arteries in man. Yasagil MG, editor. Microsurgery Applied to Neurosurgery. Stuttgart: Georg Thieme;1969. p. 82–119.2. Chang CH, Choi BY. Characteristics of training materials for successful microvascular anastomosis and preclinical assessment of the surgical skills. Korean J Cerebrovasc Surg. 2007; 9:243–6.3. Lee KS, Suh JD, Han SB, Lee SJ, Choi IC, Kim IS, et al. The effect of aspirin and prostaglandin E1 on the patency of microvascular anastomosis in rat. Korean J Microsurg. 2000; 9:179–85.4. Joo YH, Sun DI, Park JO, Cho KJ, Seo JH, Park JW, et al. Analysis of recipient vessel for microvascular reconstruction of the head and neck. Korean J Otorhinolaryngol-Head Neck Surg. 2010; 53:20–3.
Article5. Kim SM, Seo MH, Kang JY, Eo MY, Myoung H, Lee SK, et al. Anatomical review of radial forearm free flap for the oral cavity reconstruction. J Korean Assoc Maxillofac Plast Reconstr Surg. 2011; 33:95–101.6. Hoballah JJ. Vascular reconstructions; anatomy, exposures, and techniques. New York: Springer;2000. p. 17–26.7. Hoballah JJ, Eid GM, Nazzal MM, Sharp WJ, Corson JD. Contralateral internal jugular vein interposition for salvage of a functioning arteriovenous fistula. Ann Vasc Surg. 2000; 14:679–82.
Article8. Rutherford RB. Atlas of vascular surgery: basic techniques and exposures. Philadelphia: Saunders;1993. p. 48–9.9. Pinheiro AL, Castro JF, Thiers FA, Cavalcanti ET, Re -go TI Quevedo AS. Using Novafil: would in make suturing easier? Braz Dent J. 1997; 8:21–5.10. Kirklin JW, Barratt-Boyes BG. Ischemic heart disease. Kirklin JW, Barratt-Boyes BG, editors. Cardiac surgery. 2nd ed.New York: Churchill-Livingstone;1993. p. 309.11. Carrel A. The operative technique of vascular anastomoses and the transplantation of viscera. Med Lyon. 1902; 98:859.12. Nakayama K, Yamamoto K, Tamiya T, Makino H, Odaka M, Ohwada M, et al. Experience with free autografts of the bowel with a new venous anastomosis apparatus. Surgery. 1964; 55:796–802.13. Sotturai VS, Batson RC. Use of nonreversed, translocated saphenous vein graft. Bergean JJ, Yao JST, editors. Techniques in arterial surgery. Philadelphia: Saunders;1990. p. 184–91.14. Taylor LM, Porter JM. Technique of reversed vein bypass to distal leg arteries. Bergean JJ, Yao JST, editors. Techniques in arterial surgery. Philadelphia: Saunders;1990. p. 109–121.15. Bergan JJ, Veith FJ, Bernhard VM, Yao JS, Flinn WR, Gupta SK, et al. Randomization of autogenous vein and polytetrafluoroethylene grafts in femoral-distal reconstructions. Surgery. 1982; 92:921–30.16. Bush HL Jr, Nabseth DC, Curl GR, O’ Hara ET, Johnson WC, Vollman RW. In situ saphenous vein bypass grafts for limb salvage. A current fad or a viable alternative to reversed vein bypass grafts? Am J Surg. 1985; 149:477–80.17. De Bakey ME, Crawford ES, Morris GC Jr, Cooley DA. Patch graft angioplasty in vascular surgery. J Cardiovasc Surg. 1962; 3:106–41.18. Fillinger MF, Kerns DB, Bruch D, Reinitz ER, Schwartz RA. Does the end-to-end venous anastomosis offer a functional advantage over the end-to-side venous anastomosis in high-output arteriovenous grafts? J Vasc Surg. 1990; 12:676–88.
Article19. Yamamoto Y, Nohira K, Kuwahara H, Sekido M, Furukawa H, Sugihara T. Superiority of end-to-side anastomosis with the internal jugular vein: the experience of 80 cases in head and neck microsurgical reconstruction. Br J Plast Surg. 1999; 52:88–91.
Article20. Ueda K, Harii K, Nakatsuka T, Asato H, Yamada A. Comparison of end-to-end and end-to-side venous anastomosis in free-tissue transfer following resection of head and neck tumors. Microsurgery. 1996; 17:146–9.
Article21. Khouri RK. Avoiding free flap failure. Clin Plast Surg. 1992; 19:773–81.
Article22. Khouri RK, Cooley BC, Kunselman AR, Landis JR, Yeramian P, Ingram D, et al. A prospective study of microvascular free-flap surgery and outcome. Plast Reconstr Surg. 1998; 102:711–21.
Article23. Kanoh N, Dai CF, Ikeda N, Mimura O. Parameters for the preoperative evaluation of arteriosclerosis for free-flap transfers in head and neck surgery. Clin Otolaryngol Allied Sci. 2000; 25:135–8.
Article24. Biemer E, Stock W, Wolfensberger C, Ingianni G, Götz WD. Successful replantation of a totally avulsed scalp. Br J Plast Surg. 1979; 32:19–21.
Article25. Höltje WJ. Successful replantation of an amputated upper lip. Plast Reconstr Surg. 1984; 73:664–70.
Article26. Mutimer KL, Banis JC, Upton J. Microsurgical reattachment of totally amputated ears. Plast Reconstr Surg. 1987; 79:535–41.
Article27. Kim JS, Choi TH, Kim NG, Lee KS, Han KH, Son DG, et al. The replantation of an amputated tongue by supermicrosurgery. J Plast Reconstr Aesthet Surg. 2007; 60:1152–55.
Article28. Sinna R, Boloorchi A, Mahajan AL, Qassemyar Q, Robbe M. What should define a “perforator flap?”Plast Reconstr Surg. 2010; 126:2258–63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Inductive or deductive? Research by maxillofacial surgeons
- Author’s reply to the letter to the editor of Journal of the Korean Association of Oral and Maxillofacial Surgeons
- Factors affecting anastomosis failure in microvascular fibula flap reconstruction of the maxillofacial region: a systematic review and meta-analysis
- Anatomical Review of Radial Forearm Free Flap for the Oral Cavity Reconstruction
- Importance of various oral manifestations regardless of CD4 cell count in HIV/AIDS patients
