Identification of Fat in Myxoid Matrix-Rich Mesenteric Lipoblastoma Using In-Phase and Opposed-Phase MRI: A Case Report
- Affiliations
-
- 1Department of Radiology, Beijing Children's Hospital Affiliated to Capital Medical University, Beijing, China.
- 2Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hwgoo@amc.seoul.kr
- KMID: 1443499
- DOI: http://doi.org/10.3348/jksr.2011.65.1.89
Abstract
- We present a rare case of a myxoid matrix-rich mesenteric lipoblastoma. In this case, fat-saturated T1-weighted magnetic resonance (MR) imaging failed to disclose the fatty component of the tumor, while in-phase and opposed-phase MR imaging could accurately identify small fat scattered in this myxoid matrix-rich tumor.
MeSH Terms
Figure
-
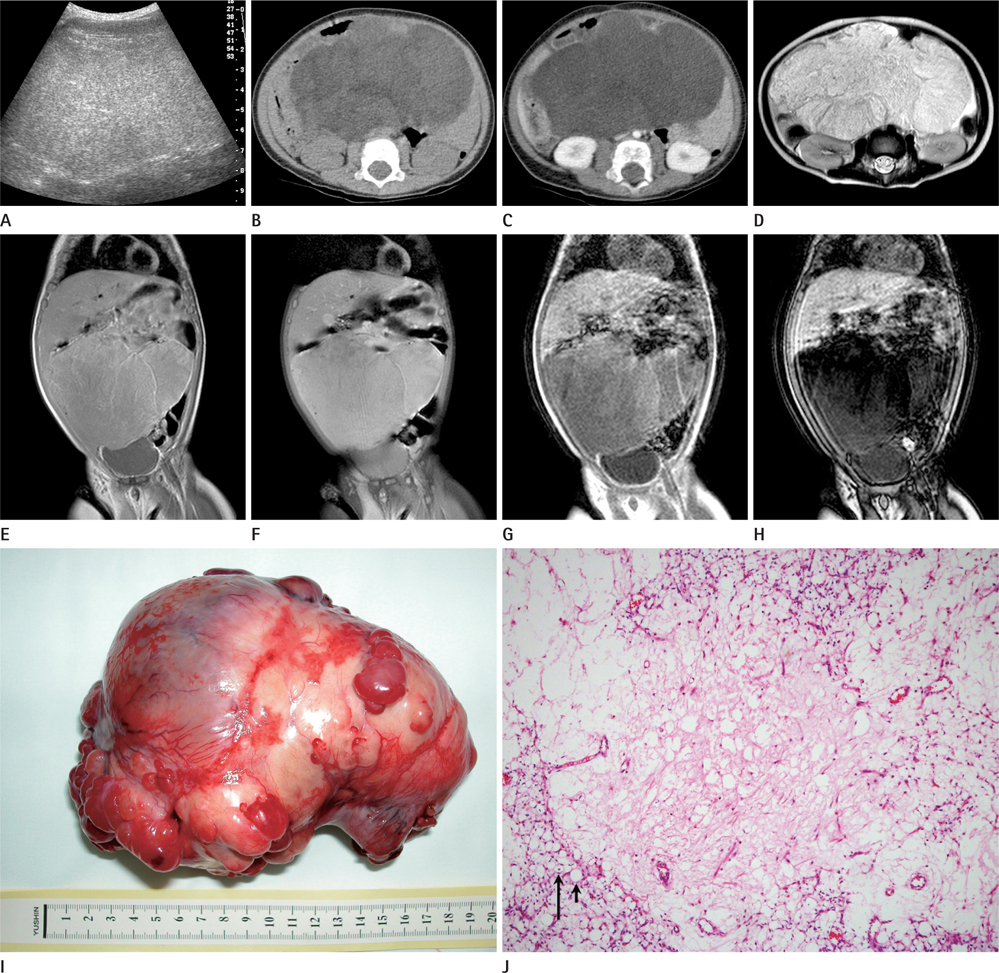
Fig. 1 Imaging and histologic findings of myxoid matrix-rich mesenteric lipoblastoma. A. Transverse abdominal US shows a large, lobulated, well-defined, hyperechoic solid mass without posterior acoustic enhancement. B. Precontrast axial CT image reveals multiple lobules of the mass with central isodensity (36 HU) and peripheral hypodensity (10 HU) and without a definite evidence of fat. C. Contrast-enhanced axial CT image demonstrates a minimal degree of enhancement (4-7 HU) in the hypodense mass. D. Axial T2-weighted MR image shows diffuse hyperintensity with hypointense septa of the mass. E. Coronal T1-weighted MR image shows diffuse isointensity with hyperintense peripheral rims of the mass. F. Coronal, fat suppressed T1-weighted MR image shows no evidence of fat suppression in the majority of the mass. G. Coronal, T1-weighted gradient-echo in-phase MR image shows a slightly hypointense mass with hyperintense peripheral rims. H. Coronal opposed-phase MR image demonstrates a considerable drop in signal intensity in the entire mass. I. Gross specimen shows that the resected mass appears bosselated, yellowish gray, and myxoid. J. Photomicrograph shows scattered immature lipoblasts (long arrow) characterized by nuclear indentation by lipid-containing cytoplasmic vacuoles, as well as a few mature adipocytes (short arrow) characterized by the crescent-shaped peripheral nucleus and a large lipid droplet in abundant myxoid matrix background (Hematoxylin & Eosin stain, × 40). Note.-MR = magnetic resonance
Reference
-
1. Bancroft LW, Kransdorf MJ, Peterson JJ, O'Connor MI. Benign fatty tumors: classification, clinical course, imaging appearance, and treatment. Skeletal Radiol. 2006; 35:719–733.2. Moholkar S, Sebire NJ, Roebuck DJ. Radiological-pathological correlation in lipoblastoma and lipoblastomatosis. Pediatr Radiol. 2006; 36:851–856.3. Mo YH, Peng SS, Li YW, Shun CT. Mesenteric lipoblastoma: case report. Pediatr Radiol. 2003; 33:37–40.4. Cudnik R, Efron PA, Chen MK, Reith JD, Beierle EA. Mesenteric lipoblastoma: a rare location in children. J Pediatr Surg. 2008; 43:e5–e7.5. Kelekis NL, Alexopoulou E, Brountzos EN, Ladis V, Boussiotou A, Kelekis DA. Giant adrenal myelolipoma with minimal fat content in a patient with homozygous beta-thalassemia: appearance on MRI. J Magn Reson Imaging. 2003; 18:608–611.6. Takahashi K, Inaoka T, Murakami N, Hirota H, Iwata K, Nagasawa K, et al. Characterization of the normal and hyperplastic thymus on chemical-shift MR imaging. AJR Am J Roentgenol. 2003; 180:1265–1269.7. Delfaut EM, Beltran J, Johnson G, Rousseau J, Marchandise X, Cotten A. Fat suppression in MR imaging: techniques and pitfalls. Radiographics. 1999; 19:373–382.8. Merkle EM, Nelson RC. Dual gradient-echo in-phase and opposed-phase hepatic MR imaging: a useful tool for evaluating more than fatty infiltration or fatty sparing. Radiographics. 2006; 26:1409–1418.9. Wang SF, Chang CY, Wu HD. Lipoblastomatosis of the shoulder: unusual MR appearance. Br J Radiol. 1998; 71:884–885.
