Dynamic Multidetector CT Findings of Left Atrial Myxomas Causing Mitral Valve Obstruction
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 2Department of Radiology, Chosun University School of Medicine, Gwangju, Korea. dhk1107@hanmail.net
- 3Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 4Department of Cardiovascular Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 5Department of Pathology, Soonchunhyang University, College of Medicine, Bucheon, Korea.
- KMID: 1443491
- DOI: http://doi.org/10.3348/jksr.2011.65.1.35
Abstract
- We report multidetector row CT (MDCT) findings of two left atrial myxomas causing mitral valve obstruction and dyspnea of patients. Cardiac MDCT showed well-defined left atrial masses attached to the interatrial septum and shifting of tumors into the left ventricle causing mitral valve obstruction during diastole in a 37-year-old male and in a 69-year-old female. Also, we observed intratumoral hemorrhage in the second case. Myxomas were resected and the patients were discharged without dyspnea.
MeSH Terms
Figure
-

Fig. 1 A 37-year-old man with typical myxoma. Chest radiograph (A) showed cardiomegaly and pulmonary vascular redistribution in the upper lungs (arrows). Four-chamber view of transesophageal echocardiography (B) shows a left atrial tumor which was attached to inter-atrial septum and prolapsed into the left ventricle. The mass caused mitral valve obstruction. Four-chamber cardiac MDCT scans (C, D) show an irregularly marginated left atrial mass abutting the inter-atrial septum with left atrial enlargement. The mass showed areas of hypoattenuation relative to intra-atrial blood. In systole (C), the mass is confined in the left atrium. However, in diastole (D), the left atrial mass protrudes into the left ventricle via the mitral valve making waist of the mass (arrows). Intraoperative specimen (E) shows several gelatinous lumps, measuring 6.5 × 5.0 × 4.5 cm. A piece of white endocardium is seen to be attached to the mass (arrow) and the external surface of the mass is smooth and glistening.
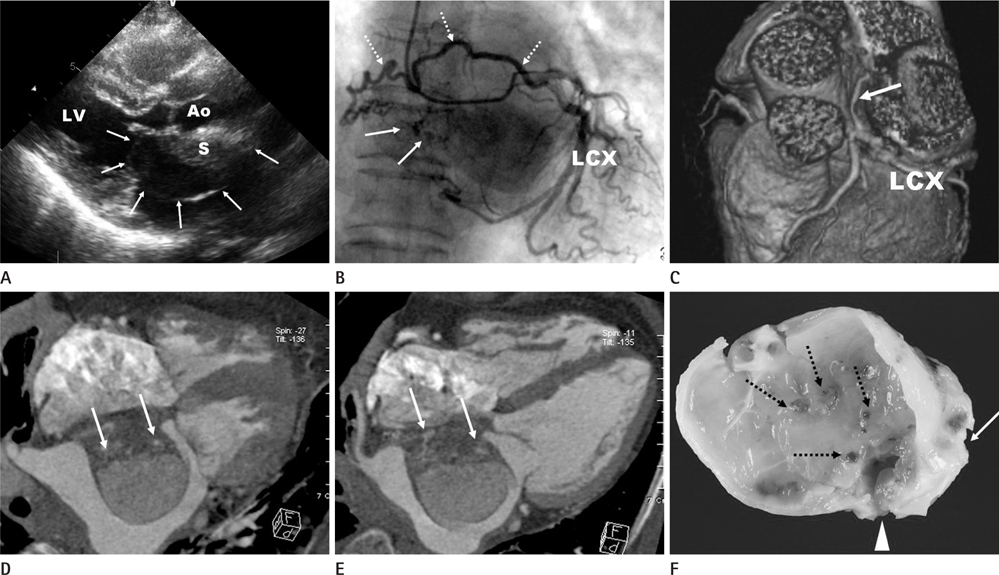
Fig. 2 A 69-year-old woman with atypical myxoma with intratumoral hemorrhage. Parasternal long-axis 2D echo image (A) at end-diastole shows the protruded cystic mass (arrows) with a solid portion (S) abutting inter-atrial septum. 'Ao' and 'LV' mean aorta and left ventricle, respectively. The coronary angiography (B) shows hypervascularity in the tumor (arrows). The feeder (dotted arrows) originated from the left circumflex artery (LCX). Also, a volume-rendering image of CT (C) shows a feeder arising from LCX (arrow). Four-chamber images of MDCT scans at end-systole (D) and end-diastole (E) show a well demarcated cystic mass attached to interatrial septum and includes mixed low attenuated (more septal portion) and hyperenhanced (more intraatrial portion) portions. The center of the more hypoattenuated portion show dot-like enhancements which are suspected of having vascular structures (arrows). A more compact mass within left atrium is seen at end-diastole (E). A photo of the gross specimen (F) show a whitish ovoid mass measuring 5.0 × 4.0 × 1.5 cm. A piece of white endocardium is seen to be attached to the mass (arrow). The external surface is lobulated, whitish myxoid, and firm. On section, the inner component of the mass is soft and whitish myxoid with hemorrhagic areas (arrow head), a glistening cut surface, and prominent vascular structures (dotted arrows). Note.-LCX = left circumflex artery, MDCT = multidetector row CT
Reference
-
1. Burke AP, Virmani R. Cardiac myxoma. A clinicopathologic study. Am J Clin Pathol. 1993; 100:671–680.2. Scheffel H, Baumueller S, Stolzmann P, Leschka S, Plass A, Alkadhi H, et al. Atrial myxomas and thrombi: comparison of imaging features on CT. AJR Am J Roentgenol. 2009; 192:639–645.3. Kim EY, Choe YH, Sung K, Park SW, Kim JH, Ko YH. Multidetector CT and MR imaging of cardiac tumors. Korean J Radiol. 2009; 10:164–175.4. Awamleh P, Alberca MT, Gamallo C, Enrech S, Sarraj A. Left atrium myxosarcoma: an exceptional cardiac malignant primary tumor. Clin Cardiol. 2007; 30:306–308.5. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001; 80:159–172.6. Gerber BL, Bluemke DA, Rumberger JA, Horton KM, Lima JAC. Cardiac imaging of masses, tumors, and thrombi. In : Sutton MG, Rutherford JD, editors. Clinical cardiovascular imaging: a companion to Braunwald's heart disease. Philadelphia: Elsevier Saunders;2004. p. 414–437.7. Chow WH, Chow TC, Tai YT, Yip AS, Cheung KL. Angiographic visualization of 'tumour vascularity' in atrial myxoma. Eur Heart J. 1991; 12:79–82.8. Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics. 2000; 20:1073–1103. quiz 1110-1111, 1112.9. Tsuchiya F, Kohno A, Saitoh R, Shigeta A. CT findings of atrial myxoma. Radiology. 1984; 151:139–143.10. Bjessmo S, Ivert T. Cardiac myxoma: 40 years' experience in 63 patients. Ann Thorac Surg. 1997; 63:697–700.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pregnancy, Paroxysmal Nocturnal Dyspnea, Presyncope, and Plop: A Case of Left Atrial Myxoma Causing Mitral Valve Obstruction in Pregnancy
- Relation between Atrial Fibrillation and Echocardiographic Size of Left Atrium
- Free-Floating Left Atrial Thrombus with Recurrent cerebral Embolic Event Associated Mitral Stenosis
- Left Atrial Wall Calcification after Mitral Valve Replacement: CT Findings and Clinical Significance
- Left Atrial Wall Dissection after Mitral Valve Replacement
