CT Demonstration of the Extracardiac Anastomoses of the Coronary Veins in Superior Vena Cava or Left Brachiocephalic Vein Obstruction
- Affiliations
-
- 1Department of Diagnostic Radiology, Montreal General Hospital, McGill University Health Centre, Montreal, Quebec H3G 1A4, Canada. joseph.casullo@muhc.mcgill.ca
- KMID: 1430057
- DOI: http://doi.org/10.3348/kjr.2013.14.1.132
Abstract
- CT scans in four cases of chronic superior vena cava or left brachiocephalic vein obstruction demonstrate a systemic-to-cardiac collateral venous pathway through anastomoses between the pericardial branches of systemic veins and the presumed adventitial veins of the ascending aorta and pulmonary trunk. These adventitial veins then drain into tributaries of the anterior cardiac veins or ventricular coronary veins.
Keyword
MeSH Terms
Figure
-

Fig. 1 CT angiogram of 70 year old male with metastatic renal cell carcinoma and obstruction of superior vena cava. A. Transverse image through thorax at level of upper limit of pericardium shows occlusion of superior vena cava by metastatic adenopathy (*) and extensive network of venous collaterals (long white arrows) in mediastinum. Note early opacification of pulmonary vein (curved white arrow) in left lung through systemic-to-pulmonary venous anastomoses (not shown) across pleural thickening (short white arrow) and probable adhesions from remote left lower lobectomy. A, B. Pericardial veins (arrowheads in A) at anterior aspect of ascending aorta and pulmonary trunk are continuous with small vessels (arrows in B) along intrapericardial portions of great arteries. C. At root of ascending aorta and base of pulmonary trunk, collateral vessels (black arrows) spread along left coronary artery (arrowhead) and its branches and drain into anterior interventricular vein (white arrows). Latter also receives collateral vessel (curved arrow) directly from left lateral wall of pulmonary trunk. D. Slightly more inferiorly, collateral vessel (long white arrow) drains into left coronary vein (short white arrow). On right, collateral branches (black arrows) pass anteriorl or posteriorl to right coronary artery (arrowhead) on their way to right atrial appendage (RAA). E. At lower level, there is early opacification of left coronary vein (short white arrow), and focal collections of contrast are present in wall of right atrial appendage (arrowheads). Collateral vessel (black arrow) posterior to right coronary artery (curved arrow) made loop inferiorly (not shown) before emptying into right auricular wall (black arrowhead). Collateral vessel situated anterior to coronary artery in D drained into wall of appendage more anteriorly (white arrowhead). P = pericardium
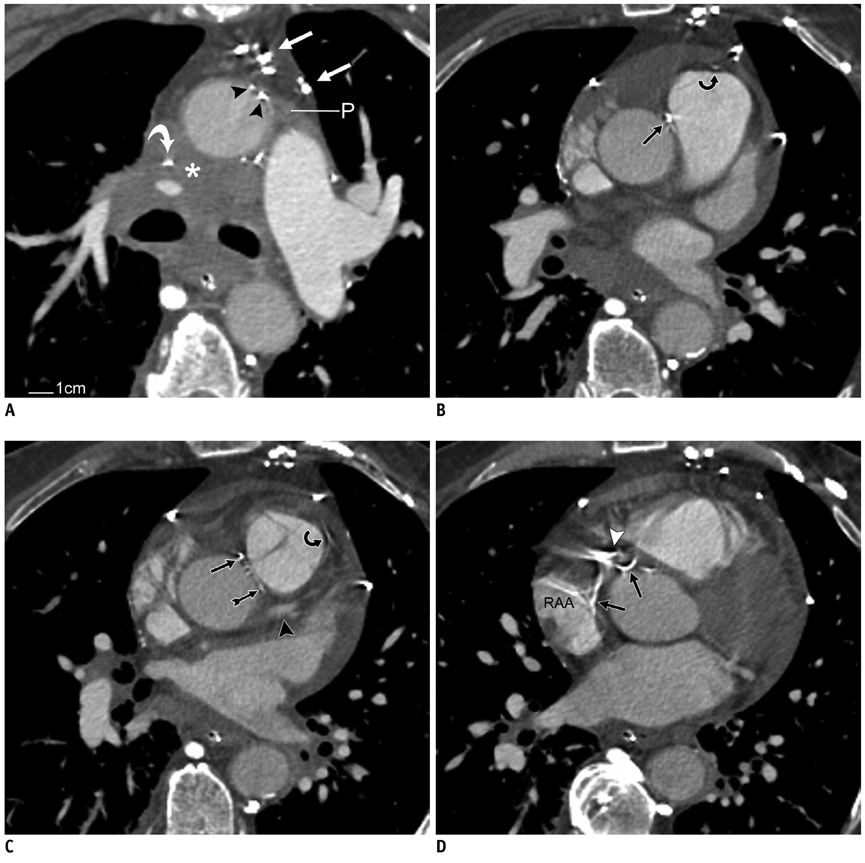
Fig. 2 CT angiogram of 71 year old male with metastatic lung carcinoma and obstruction of superior vena cava. A. Transverse image through thorax at level of upper limit of pericardium (P) shows almost complete occlusion of superior vena cava (curved white arrow) by metastatic adenopathy (*) and associated venous collaterals (straight white arrows) in anterior mediastinum. A, B. Pericardial branches (arrowheads in A) at anterior aspect of ascending aorta are continuous with small epicardial vessels in aortopulmonary groove (straight black arrow in B) and along pulmonary trunk anteriorly (curved black arrow in B). C. At level of left coronary artery (black arrowhead), collateral vessels from lateral wall of pulmonary trunk (curved black arrow) and within posterior aspect of aortopulmonary groove (feathered black arrow) could not be followed further due to image-degrading pulsation artifacts. Vessel (straight black arrow) in anterior aspect of aortopulmonary groove descends towards right atrium. D. More inferiorly, collateral vessel (black arrows) from anterior aspect of aortopulmonary groove (straight black arrow C) passes posterior to calcified right coronary artery (white arrowhead) before connecting with right atrial appendage (RAA).

Fig. 3 CT angiogram of 70 year old male with acute chest pain and remote aortocoronary bypass and surgical ligation of left brachiocephalic vein. A. Transverse image through thorax at level of aortic arch shows narrowed end of left brachiocephalic vein (curved white arrow) just before occlusion by two surgical clips (curved black arrow). There is extensive network of venous collaterals (straight white arrows) in mediastinum. B, C. Pericardial veins (arrowheads in B) around great arteries are continuous with small vessels (black arrows in C) along intrapericardial segments of ascending aorta and pulmonary trunk. Pericardium (P) was not seen anteriorly and was thin laterally. D, E. At base of great arteries, there is early opacification of left coronary vein (short white arrow in E) by collateral vessels (black arrows) from lateral wall of pulmonary trunk and posterior wall of ascending aorta. Collateral vessel from anterior wall of aorta gives off branches that accompany right coronary artery (curved white arrow) on their way to right atrial appendage (RAA). Black arrowhead in D points to left coronary artery. F. More inferiorly, collateral vessel (upper black arrow) contacts anterior surface of right atrial appendage. F, G. Collateral vessel along anterior wall of ascending aorta (lower black arrow in F and arrow in G) descends to aortic root where it forms loop posteriorly and connects with anterosuperior wall of left atrium (arrowheads). Image in G is reformatted CT image of chest in oblique sagittal plane. RA = right atrium, LA = left atrium, Ao = ascending aorta

Fig. 4 Reformatted CT image of chest, in oblique coronal plane, of 66 year old male with catheter-related thrombosis (*) of left brachiocephalic vein (short white arrow). Level shown is through ascending aorta and innominate artery. At pericardial attachment to ascending aorta (black arrowhead), there is continuity between pericardial vein (long white arrow) and longitudinal vessel (long black arrow) along intrapericardial portion of ascending aorta near aortopulmonary groove (white arrowhead). Vessel passes posterior to right coronary artery (curved black arrow) before draining into right atrial appendage (not shown). Pericardial vein in question was branch of venous plexus joining left (curved white arrow) and right inferior thyroid veins. P = pericardium
Reference
-
1. Cihangiroglu M, Lin BH, Dachman AH. Collateral pathways in superior vena caval obstruction as seen on CT. J Comput Assist Tomogr. 2001. 25:1–8.2. Kapur S, Paik E, Rezaei A, Vu DN. Where there is blood, there is a way: unusual collateral vessels in superior and inferior vena cava obstruction. Radiographics. 2010. 30:67–78.3. Haller A von. First lines of physiology. A reprint of the 1786 edition. Sources of science; series no. 32. 1966. New York: Johnson Reprint Corp;49.4. Baroldi G, Scomazzoni G. Coronary circulation in the normal and the pathologic heart. 1965. Washington, DC: Armed Forces Institute of Pathology;79.5. Clarke JA. An X-ray microscopic study of the vasa vasorum of the normal human ascending aorta. Br Heart J. 1965. 27:99–104.6. Clarke JA. An x-ray microscopic study of the vasa vasorum of the normal human pulmonary trunk. Acta Anat (Basel). 1965. 61:6–14.7. Schaffler GJ, Groell R, Peichel KH, Rienmüller R. Imaging the coronary venous drainage system using electron-beam CT. Surg Radiol Anat. 2000. 22:35–39.8. Ortale JR, Marquez CQ. Anatomy of the intramural venous sinuses of the right atrium and their tributaries. Surg Radiol Anat. 1998. 20:23–29.9. von Lüdinghausen M, Ohmachi N, Besch S, Mettenleiter A. Atrial veins of the human heart. Clin Anat. 1995. 8:169–189.10. Sugiyama H, Yoo SJ, Williams W, Benson LN. Characterization and treatment of systemic venous to pulmonary venous collaterals seen after the Fontan operation. Cardiol Young. 2003. 13:424–430.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Double Left Brachiocephalic Veins with Persistent Left Superior Vena Cava: A Case Report
- Circumaortic Left Brachiocephalic Vein: CT Findings
- A Case of Behcet's Disease with Superior Vena Cava Syndrome
- Bypass of Superior Vena Cava with Spiral Vein Graft
- A Case of the Malformation of Azygos and Hemiazygos System
