A Case of Odontogenic Orbital Cellulitis Causing Blindness by Severe Tension Orbit
- Affiliations
-
- 1Department of Ophthalmology, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea. laty@catholic.ac.kr
- KMID: 1429218
- DOI: http://doi.org/10.3346/jkms.2013.28.2.340
Abstract
- We report a very rare case of odontogenic orbital cellulitis causing blindness by severe tension orbit. A 41-yr old male patient had visited the hospital due to severe periorbital swelling and nasal stuffiness while he was treated for a periodontal abscess. He was diagnosed with odontogenic sinusitis and orbital cellulitis, and treated with antibiotics. The symptoms were aggravated and emergency sinus drainage was performed. On the next day, a sudden decrease in vision occurred with findings of ischemic optic neuropathy and central retinal artery occlusion. Deformation of the eyeball posterior pole into a cone shape was found from the orbital CT. A high-dose steroid was administered immediately resulting in improvements of periorbital swelling, but the patient's vision had not recovered. Odontogenic orbital cellulitis is relatively rare, but can cause blindness via rapidly progressing tension orbit. Therefore even the simplest of dental problems requires careful attention.
Keyword
MeSH Terms
-
Adult
Anti-Bacterial Agents/adverse effects/therapeutic use
Blindness/*diagnosis/etiology
Drainage
Fluorescein Angiography
Humans
Male
Optic Neuropathy, Ischemic/complications
Orbit/*physiopathology
Orbital Cellulitis/*diagnosis
Retinal Artery Occlusion/complications
Sinusitis/diagnosis/drug therapy
Tomography, X-Ray Computed
Tooth Root
Anti-Bacterial Agents
Figure
-
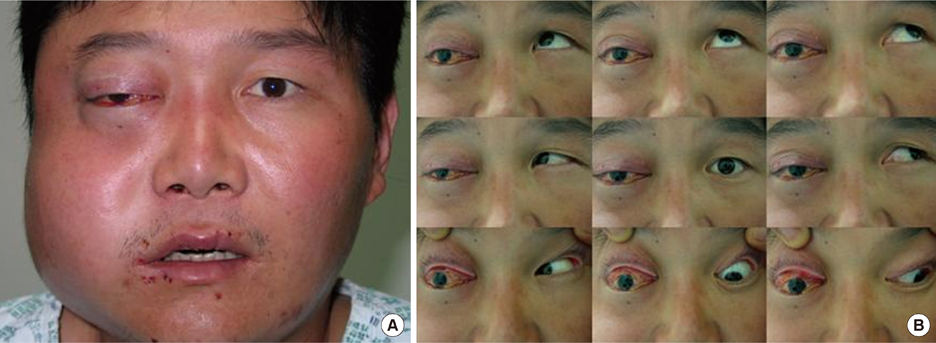
Fig. 1 Photographs of the patient's face. (A) The face showed marked swelling of right cheek and periorbital area involving eyelid, severe proptosis of the right eye. (B) Nine cardinal gaze photographs showed severe limitation of the right eyeball movement for all gazes except abduction.

Fig. 2 CT findings of the patient. (A) Coronal CT scan at presentation showed severe maxillary and ethmoidal sinusitis as well as marked inflammatory swelling of soft tissue in the right cheek and temporal region. Intraorbital soft tissue inflammation and thickening of the lateral rectus muscle of right eye were also observed. (B) Axial CT scan taken 1 day after sinus surgery showed severe tenting of the posterior part of globe (arrow) and stretching of the optic nerve due to severe proptosis.

Fig. 3 Fundus findings of the patient. (A) Fundus photograph of the right eye showed a pale optic disc, cherry red spot in macula, and edema at the posterior pole. (B) Fluorescein angiography of right eye showed a delay of retinal circulation.

Fig. 4 Swelling of the cheek and proptosis of the right eye had nearly subsided after 2 weeks of hospitalization but visual loss had not been recovered.
Reference
-
1. Mancuso AA, Hanafee WN. Mancuso AA, Verbist BM, Hermans R, editors. Tension orbit and its acute threat to vision. Head and Neck Radiology. 2010. Philadelphia: Lippincott Williams & Wilkins;62–65.2. Youssef OH, Stefanyszyn MA, Bilyk JR. Odontogenic orbital cellulitis. Ophthal Plast Reconstr Surg. 2008. 24:29–35.3. Brook I. Sinusitis of odontogenic origin. Otolaryngol Head Neck Surg. 2006. 135:349–355.4. Thakar M, Thakar A. Odontogenic orbital cellulitis. Report of a case and consideration on route of spread. Acta Ophthalmol Scand. 1995. 73:470–471.5. Poon TL, Lee WY, Ho WS, Pang KY, Wong CK. Odontogenic subperiosteal abscess of orbit: a case report. J Clin Neurosci. 2001. 8:469–471.6. Bullock JD, Fleishman JA. Orbital cellulitis following dental extraction. Trans Am Ophthalmol Soc. 1984. 82:111–133.7. Brook I. Microbiology of acute and chronic maxillary sinusitis associated with an odontogenic origin. Laryngoscope. 2005. 115:823–825.8. Nash D, Wald E. Sinusitis. Pediatr Rev. 2001. 22:111–117.9. Brook I. Microbiology of acute sinusitis of odontogenic origin presenting with periorbital cellulitis in children. Ann Otol Rhinol Laryngol. 2007. 116:386–388.10. Cho HS, Kwon JW, Ahn HS. Central reinal artery occlusion and orbital abscess following dental abscess. J Korean Ophthalmol Soc. 2003. 44:750–754.11. Dolman PJ, Glazer LC, Harris GJ, Beatty RL, Massaro BM. Mechanisms of visual loss in severe proptosis. Ophthal Plast Reconstr Surg. 1991. 7:256–260.12. Chang KC. Orbital cellulitis with subperiosteal abscess secondary to dental extraction. J Korean Ophthalmol Soc. 2008. 49:1845–1849.13. Cheon HC, Park JM, Lee JH, Ahn HB. Effect of corticosteroids in the treatment of orbital cellulitis with subperiosteal abscess. J Korean Ophthalmol Soc. 2006. 47:2030–2034.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The various orbital infections from odontogenic origin
- A Case of Orbital Infarction Syndrome in Rhino-Orbitocerebral Mucormycosis
- A Case ef Orbital Cellulitis Subdural Subdural Abscess
- A Case of Deep Neck Infecton Followed by Orbital Cellulitis
- Retinoblastoma Manifested by Hyphema and Orbital Cellulitis
