Korean J Neurotrauma.
2013 Apr;9(1):27-29. 10.13004/kjnt.2013.9.1.27.
Combined Atlantoaxial Rotatory Fixation and Unilateral Counter Occipitoatlantal Subluxation after Minor Trauma
- Affiliations
-
- 1Department of Neurosurgery, Wallace Memorial Baptist Hospital, Busan, Korea. cha7128@hanmail.net
- KMID: 1427760
- DOI: http://doi.org/10.13004/kjnt.2013.9.1.27
Abstract
- Rotatory fixation of the atlantoaxial joint is relatively rare in adults but somewhat more common in children. Most of them are reduced spontaneously or after traction. However, combined rotatory injury of atlantoaxial joint and unilateral occipitoatlantal subluxation is a rare disease, and it is often difficult to diagnose accurately. Because the craniovertebral junction is complex and patients with combined atlantoaxial rotatory fixation (AARF) and occipitoatlantal subluxation has a less rotated head than patients with pure AARF. And injury of the occipitoatlantal and atlantoaxial joint can often result upper cervical instability, so early diagnosis is very important. We present a case of the combined AARF and unilateral counter occipitoatlantal subluxation after minor trauma.
MeSH Terms
Figure
-

FIGURE 1. A: Three-dimensional CT scans showing the atlantoaxial rotatory subluxation with 26 degrees. B: C1 turned to the left and subluxation with 14 degrees on the occipital condyle. OC: occipital condyle.
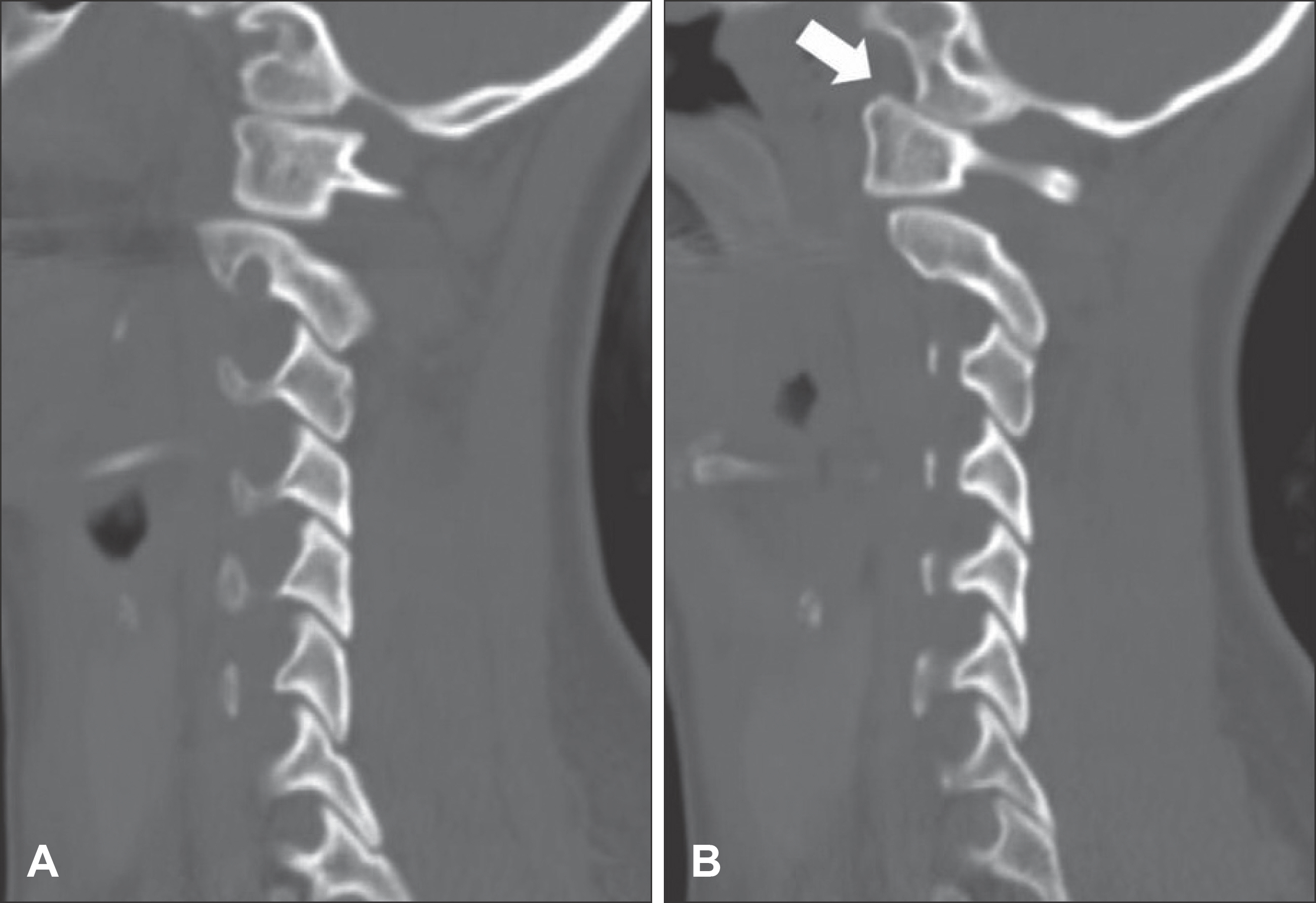
FIGURE 2. A: Left parasagittal CT reconstruction showing good articular congruence between the condyle and the lateral mass of C1. B: Right parasagittal CT reconstruction showing posterior dislocation of the condyle on the lateral mass of C1 (arrow).
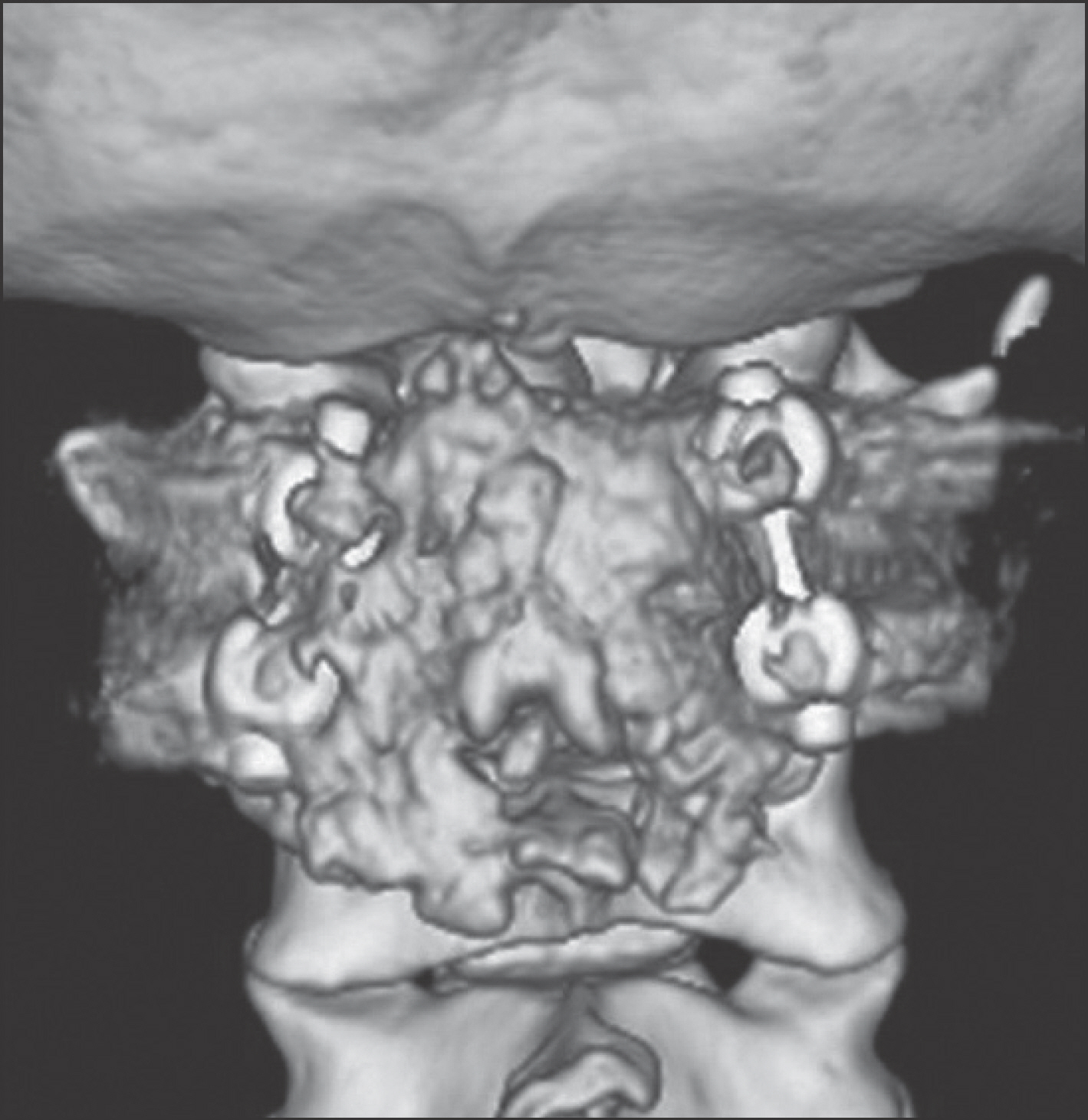
FIGURE 3. Posterative three-dimensional CT scan (posterior view). Satisfactory reduction has been accomplished and arthrodesis at C1-C2 has been performed in which allogenic bone chips.

FIGURE 4. Postoperative plain X-ray film (lateral view) showing fusion between C1 and C2.
Reference
-
References
1. Altongy JF, Fielding JW. Combined atlantoaxial and occipitoatlantal rotatory subluxation. A case report. J Bone Joint Surg Am. 72:923–926. 1990.
Article2. Bouillot P, Fuentes S, Dufour H, Manera L, Grisoli F. Imaging features in combined atlantoaxial and occipitoatlantal rotatory subluxation: a rare entity. Case report. J Neurosurg 90 (2 Suppl):258–260. 1999.3. Clark CR, Kathol MH, Walsh T, el-Khoury GY. Atlantoaxial rotatory fixation with compensatory counter occipitoatlantal subluxation. A case report. Spine (Phila Pa 1976). 11:1048–1050. 1986.4. Crossman JE, David K, Hayward R, Crockard HA. Open reduction of pediatric atlantoaxial rotatory fixation: longterm outcome study with functional measurements. J Neurosurg 100 (3 Suppl Spine):235–240. 2004.
Article5. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlantoaxial joint). J Bone Joint Surg Am. 59:37–44. 1977.6. Washington ER. Non-traumatic atlanto-occipital and atlantoaxial dislocation; a case report. J Bone Joint Surg Am 41-A:341–344. 1959.7. Wortzman G, Dewar FP. Rotary fixation of the atlantoaxial joint: Rotational atlantoaxial subluxation. Radiology. 90:479–487. 1968.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Morphologically Atypical Case of Atlantoaxial Rotatory Subluxation
- A Spontaneous Atlantoaxial Subluxation: A case repor
- Role of the O-arm and Computer-assisted Navigation of Safe Screw Fixation in Children with Traumatic Rotatory Atlantoaxial Subluxation
- The Treatment of Traumatic Atlantoaxial Rotatory Subluxation (Fielding Type I) and the Correlation between the Clinical Progress and Radiological Reduction Parameter
- Torticollis and Atlantoaxial Rotatory Subluxation after Chiropractic Therapy
