Clin Orthop Surg.
2012 Jun;4(2):163-166. 10.4055/cios.2012.4.2.163.
Augmentation with Transcortical Wiring of an Onlay-type Prosthesis for a Deficient Patella during Revision Total Knee Arthroplasty
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. heavystone75@gmail.com
- KMID: 1383879
- DOI: http://doi.org/10.4055/cios.2012.4.2.163
Abstract
- The management of patellae with a severe bony deficiency during revision total knee arthroplasty is a challenging problem. However, using a technique of augmentation with transcortical wiring of an onlay-type prosthesis allowed the authors to revise a deficient patellae successfully. After making the decision to revise the existing patellar component, the procedure was found to be technically straightforward. Furthermore, the procedure does not require sophisticated instruments, only an onlay-type prosthesis, cement and wires. This technique entails fixing wires to the three pegs of the patellar component, passing the wires through drill holes in the anterior cortex and, after compression of a cemented prosthesis, augmenting the fixation by twisting the wires anteriorly. We believe that stable fixation and painless articulation will be obtained with the described technique for deficient patellae.
MeSH Terms
Figure
-

Fig. 1 Wires are wound around each peg.
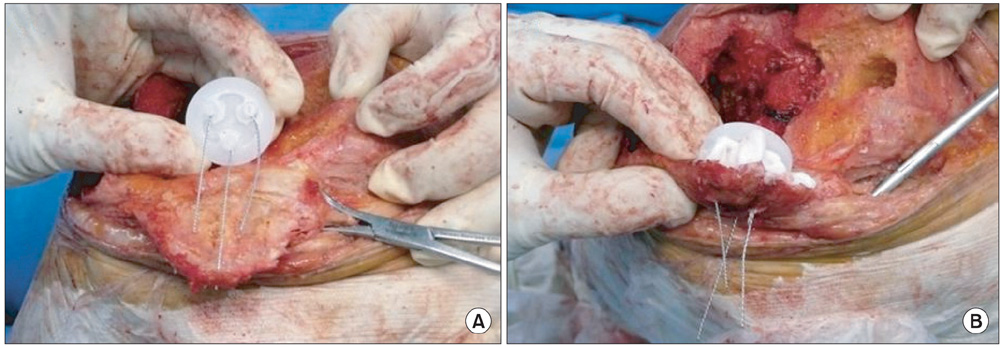
Fig. 2 (A) Wires are passed from the undersurface of the patella to the outer surface through the bone holes. (B) The space between the bone bed and the patellar component is filled with cement.
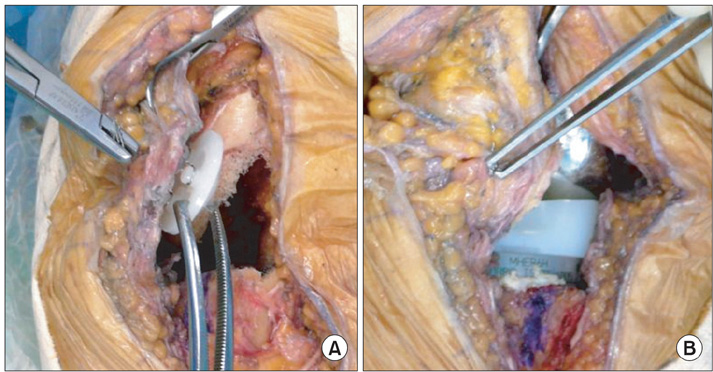
Fig. 3 (A) Enough tension is applied to the three wires placed on the outer surface using wire holders. (B) The wires are then twisted immediately above the cortex.
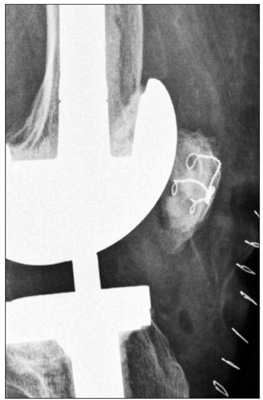
Fig. 4 Lateral view of the knee was taken immediately after surgery.

Fig. 5 Tangential view of the patella was taken 2 months after surgery.
Reference
-
1. Rorabeck CH, Mehin R, Barrack RL. Patellar options in revision total knee arthroplasty. Clin Orthop Relat Res. 2003. (416):84–92.
Article2. Maheshwer CB, Mitchell E, Kraay M, Goldberg VM. Revision of the patella with deficient bone using a biconvex component. Clin Orthop Relat Res. 2005. 440:126–130.
Article3. Nasser S, Poggie RA. Revision and salvage patellar arthroplasty using a porous tantalum implant. J Arthroplasty. 2004. 19(5):562–572.
Article4. Nelson CL, Lonner JH, Lahiji A, Kim J, Lotke PA. Use of a trabecular metal patella for marked patella bone loss during revision total knee arthroplasty. J Arthroplasty. 2003. 18:7 Suppl 1. 37–41.
Article5. Rand JA. Treatment of the patella at reimplantation for septic total knee arthroplasty. Clin Orthop Relat Res. 2003. (416):105–109.
Article6. Hanssen AD. Bone-grafting for severe patellar bone loss during revision knee arthroplasty. J Bone Joint Surg Am. 2001. 83(2):171–176.
Article7. Klein GR, Levine HB, Ambrose JF, Lamothe HC, Hartzband MA. Gull-wing osteotomy for the treatment of the deficient patella in revision total knee arthroplasty. J Arthroplasty. 2010. 25(2):249–253.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periprosthetic Fractures Following Total Knee Arthroplasty
- The Results of Revision Total Knee Arthroplasty
- Availability of Patella Resurfacing in Primary Total Knee Arthroplasty Through Evaluation and Analysis of the Patella in Revision Total Knee Arthroplasty
- Diagnosis, Causes and Treatments of Instability Following Total Knee Arthroplasty
- Delayed Repair with Augmentation using Achilles Allograft of Old Ruptured Patellar Tendon after Revison Total Knee Arthroplasty: A Case Report
