A Case of Chylopericardium Secondary to the Superior Vena Cava Syndrome in Behcet's Disease
- Affiliations
-
- 1Department of Internal Medicine, Daegu Fatima Hospital, Daegu, Korea. gunwoo@fatima.or.kr
- 2Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
- KMID: 1270205
- DOI: http://doi.org/10.4078/jkra.2008.15.3.255
Abstract
- Behcet's disease (BD) is a chronic inflammatory disorder associated with oral aphthous ulcer, genital ulcer and uveitis. Vascular lesions in BD can affect all types and sizes of vessels. The venous thrombosis, which is uncommon feature of other vasculitis, is relatively common clinical manifestation of BD. Sometimes the cardiovascular involvement in BD results in serious complications as the leading cause of morbidity and mortality. We report a 41-year-old male patient who suffered BD and presented massive chylopericardium due to the superior vena cava (SVC) syndrome. After thrombectomy of SVC, the highly productive left-sided chylothorax and restenosis of anastomosis site at SVC had occurred, which were successfully treated by the ligation of the thoracic duct and balloon-stent angioplasty. We discussed the mechanism and treatment of chylopericardium in SVC syndrome, and the possible complications after the surgical management.
Figure
-
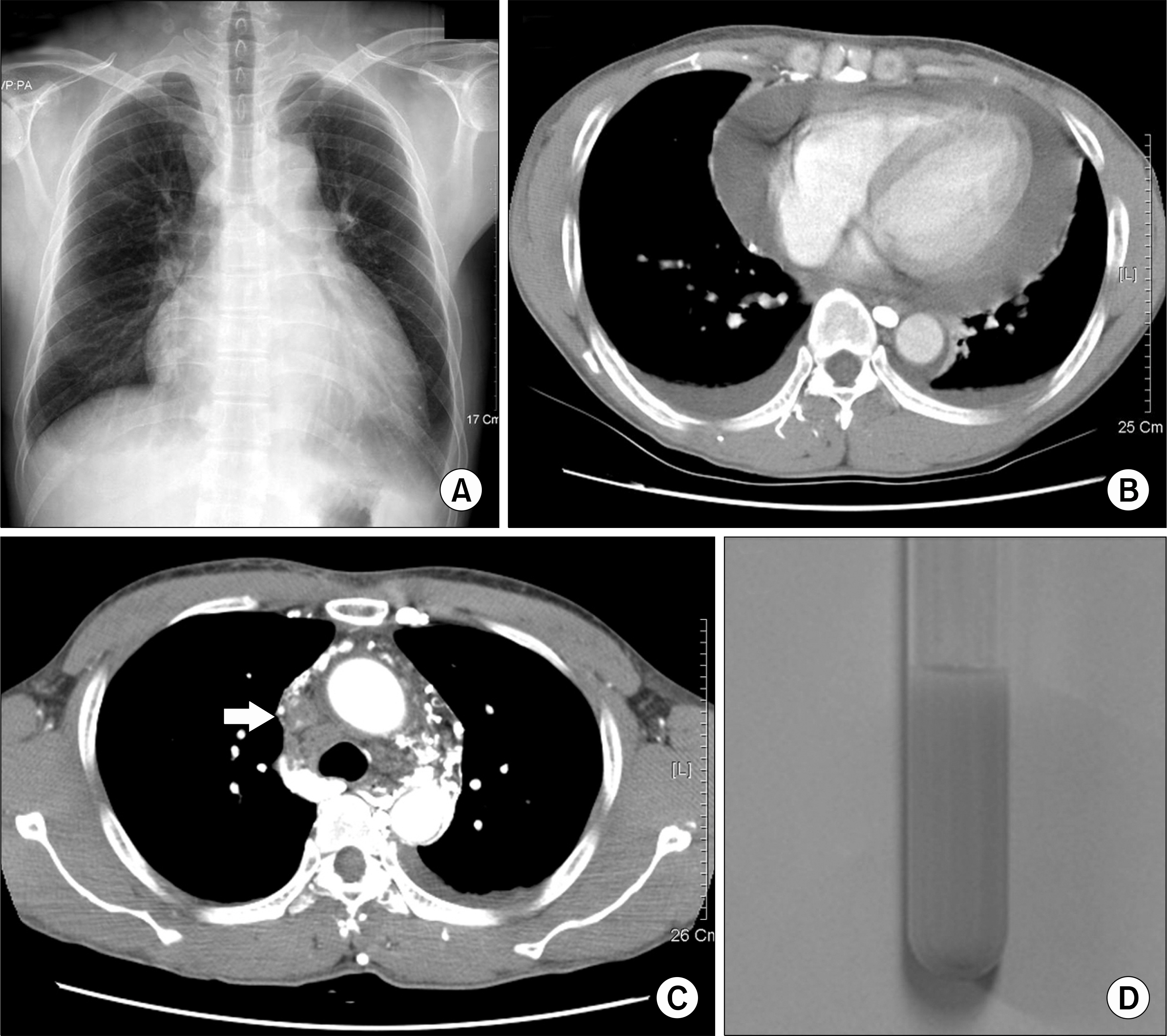
Fig. 1. Chest X-ray at admission showed enlargement of the cardiac shadow and blunting of both costophrenic angle (A). Computed tomography (CT) of chest revealed large pericardial effusion and both pleural effusion (B), and there was total thrombotic occlusion at below level of aortic arch (arrow) (C). We obtained chylous fluid by pericardiocentesis (D).

Fig. 2. The chest X-ray, carried out at 6 days after thrombectomy of SVC, showed blunting of the left sided costophrenic angle (A). On the CT angiogram, the SVC had a marked reduction in the lumen (arrow head) and the left brachiocephalic vein showed total occlusion (arrow) with prominent collateral vessels (B).
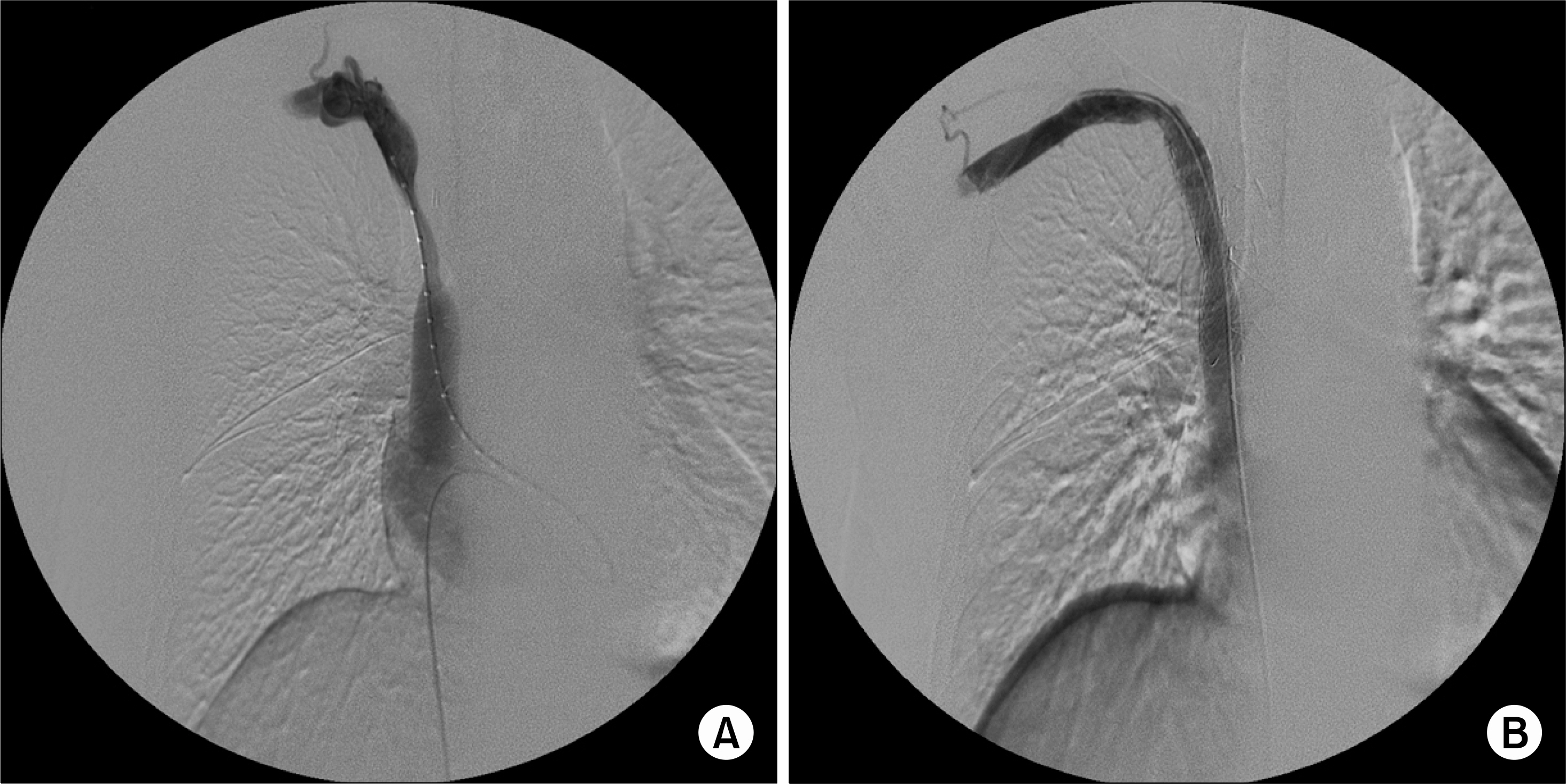
Fig. 3. Cavography showed the severe narrowing of the SVC (A). After the stent insertion with ballooning, the stenosis was disappeared and blood flow was restored (B).
Reference
-
References
1. Yazici H, Fresko I, Yurdakul S. Behcet's syndrome: disease manifestations, management, and advances in treatment. Nat Clin Pract Rheumatol. 2007; 3:148–55.2. Calamia KT, Schirmer M, Melikoglu M. Major vessel involvement in Behcet disease. Curr Opin Rheumatol. 2005; 17:1–8.3. Han SW, Kang YM, Kim YW, Lee JT. Cardiovascular involvement in Behcet's disease. Korean J Med. 2003; 64:542–51.4. Cho BC, Kang SM, Lee SC, Moon JG, Lee DH, Lim SH. Primary idiopathic chylopericardium associated with cervicomediastinal cystic hygroma. Yonsei Med J. 2005; 46:439–44.
Article5. Coplu L, Emri S, Selcuk ZT, Kalyoncu F, Balkanci F, Sahin AA, et al. Life threatening chylous pleural and pericardial effusion in a patient with Behcet's syndrome. Thorax. 1992; 47:64–5.
Article6. Oz N, Sarper A, Erdogan A, Demircan A, Isin E. Video-assisted thoracic surgery for the management of pleural and pericardial effusion in Behcet's syndrome. Tex Heart Inst J. 2000; 27:304–6.7. Moon H, Lee YJ, Lee SI, Yoo WH. Chylothorax and chylopericardium as the initial clinical manifestation of Behcet's disease. Rheumatol Int. 2008; 28:375–7.
Article8. Castelli P, Caronno R, Piffaretti G, Tozzi M, Lomazzi C, Lagana D, et al. Endovascular treatment for superior vena cava obstruction in Behcet disease. J Vasc Surg. 2005; 41:548–51.9. Wang CH, Yen TC, Ng KK, Lee CM, Hung MJ, Cherng WJ. Pedal (99m)Tc-sulfur colloid lymphoscintigraphy in primary isolated chylopericardium. Chest. 2000; 117:598–601.
Article10. Haznedaroglu IC, Celik I, Buyukasik Y, Kosar A, Kirazli S, Dundar SV. Haemostasis, thrombosis, and endothelium in Behcet's disease. Acta Haematol. 1998; 99:236–7.
Article11. Nah SS, Hong SC, Lee CK, Oh JS, Kim YG, Jeon CH, et al. Effect of Immunosuppressive agents on recurrence of cardiovascular involvement of Behcet's disease. J Korean Rheum Assoc. 2007; 14:345–53.
Article12. Hartung O, Benmiloud F, Barthelemy P, Dubuc M, Boufi M, Alimi YS. Late results of surgical venous thrombectomy with iliocaval stenting. J Vasc Surg. 2008; 47:381–7.
Article13. Han SW, Kim GW, Lee J, Kim YJ, Kang YM. Successful treatment with stent angioplasty for Budd-Chiari syndrome in Behcet's disease. Rheumatol Int. 2005; 25:234–7.14. Kalra M, Gloviczki P, Andrews JC, Cherry KJ Jr, Bower TC, Panneton JM, et al. Open surgical and endovascular treatment of superior vena cava syndrome caused by nonmalignant disease. J Vasc Surg. 2003; 38:215–23.
Article15. Chang JH, Koh MB, Shin DI, Kwok SK, Cho BS, Kim WU, et al. Superior vena cava thrombosis treated successfully by percutaneous insertion of metallic stent in a patient with Behcet's disease. J Korean Rheum Assoc. 2002; 9:230–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Behcet's Disease with Superior Vena Cava Syndrome
- A case of Behcet's syndrome with superior vena cava syndrome
- Superior Vena Cava Thrombosis Treated Successfully by Percutaneous Insertion of Metallic Stent in a Patient with Behcet's Disease
- A Case of Superior Vena Cava Syndrome
- A Case of Behcet's Syndrome with Superior Vena Cava Obstruction and Massive Pericardial Effusion
