Korean J Radiol.
2012 Apr;13(2):144-151. 10.3348/kjr.2012.13.2.144.
Cumulative Radiation Exposure during Follow-Up after Curative Surgery for Gastric Cancer
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Severance Hospital, Yonsei University College of Medicine, Seoul 120-752, Korea. yelv@yuhs.ac
- 2Department of Emergency Medicine, Yonsei University College of Medicine, Seoul 120-752, Korea.
- KMID: 1245378
- DOI: http://doi.org/10.3348/kjr.2012.13.2.144
Abstract
OBJECTIVE
To quantify the cumulative effective dose (cED) of radiation due to repeated CT and PET/CT examinations after curative resection of gastric cancer and to assess the lifetime attributable risk (LAR) estimates based on Biological Effects of Ionizing Radiation VII models.
SUBJECTS AND METHODS
Patients who underwent a curative resection for gastric cancer between January 2006 and December 2006 and were followed-up until May 2010 were included in this study. The cED was calculated by using the dose-length product values and conversion factors for quantitative risk assessment of radiation exposure. cED and LAR were compared between early and advanced gastric cancer patients and among American Joint Committee on Cancer TNM stage groups (stage I, II, and III). The nonparametric Mann-Whitney U and Kruskal-Wallis tests, followed by a post-hoc analysis with Bonferroni adjustment, were employed as part of the statistical analysis.
RESULTS
The overall median cED was 57.8 mSv (interquartile range [IQR], 43.9-74.7). The cED was significantly higher in the advanced (median, 67.0; IQR, 49.1-102.3) than in the early gastric cancer group (median, 52.3; IQR, 41.5-67.9) (p < 0.001), and increased as the TNM stage increased. For radiation exposure, 62% of all patients received an estimated cED of over 50 mSv, while 11% of patients received over 100 mSv. The median LAR of cancer incidence was 0.28% (IQR, 0.20-0.40) and there were significant differences between the early gastric cancer and advanced gastric cancer group (p < 0.001) as well as among the three TNM stage groups (p = 0.015). The LAR of cancer incidence exceeded 1% in 2.4% of the patients.
CONCLUSION
The cED increases proportionally along with tumor stage and, even in early gastric cancer or stage I patients, cED is much higher than that found among the general population. Considering the very good prognosis of early gastric cancer after curative surgery, the cED should be considered when designing a postoperative follow-up CT protocol.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Female
Follow-Up Studies
Gastrectomy
Humans
Male
Middle Aged
Neoplasm Staging
*Positron-Emission Tomography and Computed Tomography
*Radiation Dosage
Retrospective Studies
Risk Assessment
Statistics, Nonparametric
Stomach Neoplasms/pathology/*radiography/*radionuclide imaging/surgery
*Tomography, X-Ray Computed
Treatment Outcome
Figure
-
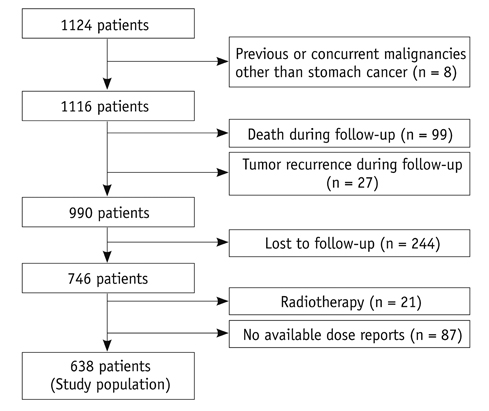
Fig. 1 Flow chart of patient inclusion, with reason for exclusion and total study population.
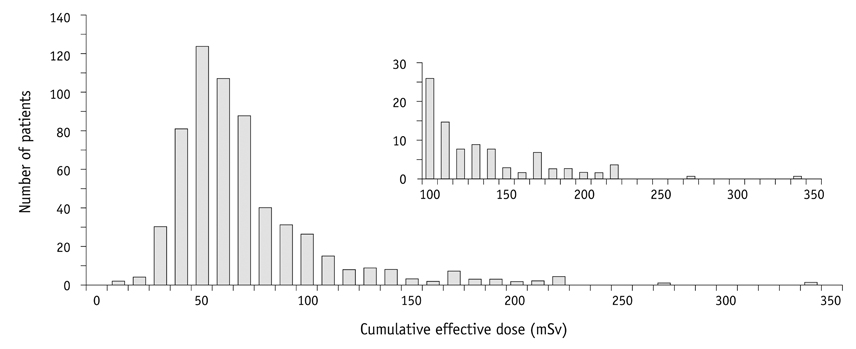
Fig. 2 Histogram of cumulative CT effective dose per patient. Inset includes expanded y-axis to display right tail and contains number of patients who received more than 100 mSv.
Reference
-
1. Edge SB. Cancer AJCo. Ajcc cancer staging manual. 2010. 7th ed. New York: Springer.2. Whiting J, Sano T, Saka M, Fukagawa T, Katai H, Sasako M. Follow-up of gastric cancer: A review. Gastric Cancer. 2006. 9:74–81.3. Park JC, Lee YC, Kim JH, Kim YJ, Lee SK, Hyung WJ, et al. Clinicopathological aspects and prognostic value with respect to age: An analysis of 3,362 consecutive gastric cancer patients. J Surg Oncol. 2009. 99:395–401.4. Hur H, Song KY, Park CH, Jeon HM. Follow-up strategy after curative resection of gastric cancer: A nationwide survey in Korea. Ann Surg Oncol. 2010. 17:54–64.5. The 2007 recommendations of the international commission on radiological protection. Icrp publication 103. Ann ICRP. 2007. 37:1–332.6. Fazel R, Krumholz HM, Wang Y, Ross JS, Chen J, Ting HH, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med. 2009. 361:849–857.7. Sodickson A, Baeyens PF, Andriole KP, Prevedello LM, Nawfel RD, Hanson R, et al. Recurrent ct, cumulative radiation exposure, and associated radiation-induced cancer risks from ct of adults. Radiology. 2009. 251:175–184.8. Chung HW, Noh SH, Lim JB. Analysis of demographic characteristics in 3242 young age gastric cancer patients in Korea. World J Gastroenterol. 2010. 16:256–263.9. Murakami T, Yasui A, Tazaki H, Hirase Y, Maeda S. [gastric cancer]. Saishin Igaku. 1971. 27:115–119.10. Office for Official Publications of the European Communities. European guidelines on quality criteria for computed tomography Luxembourg: Office for Official Publications of the European Communities. 1999.11. Brix G, Lechel U, Glatting G, Ziegler SI, Munzing W, Muller SP, et al. Radiation exposure of patients undergoing whole-body dual-modality 18f-fdg pet/ct examinations. J Nucl Med. 2005. 46:608–613.12. Association KGC. 2004 nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2007. 7:47–54.13. Kirpalani H, Nahmias C. Radiation risk to children from computed tomography. Pediatrics. 2008. 121:449–450.14. Kodera Y, Ito S, Yamamura Y, Mochizuki Y, Fujiwara M, Hibi K, et al. Follow-up surveillance for recurrence after curative gastric cancer surgery lacks survival benefit. Ann Surg Oncol. 2003. 10:898–902.15. Youn HG, An JY, Choi MG, Noh JH, Sohn TS, Kim S. Recurrence after curative resection of early gastric cancer. Ann Surg Oncol. 2010. 17:448–454.16. Renehan AG, Egger M, Saunders MP, O'Dwyer ST. Impact on survival of intensive follow up after curative resection for colorectal cancer: Systematic review and meta-analysis of randomised trials. BMJ. 2002. 324:813.17. Okines A, Verheij M, Allum W, Cunningham D, Cervantes A. Gastric cancer: Esmo clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010. 21:Suppl 5. v50–v54.18. Kim JH, Jang YJ, Park SS, Park SH, Mok YJ. Benefit of post-operative surveillance for recurrence after curative resection for gastric cancer. J Gastrointest Surg. 2010. 14:969–976.19. Park CH, Song KY, Kim SN. Treatment results for gastric cancer surgery: 12 years' experience at a single institute in Korea. Eur J Surg Oncol. 2008. 34:36–41.20. Maehara Y, Kakeji Y, Oda S, Takahashi I, Akazawa K, Sugimachi K. Time trends of surgical treatment and the prognosis for japanese patients with gastric cancer. Br J Cancer. 2000. 83:986–991.21. Nunobe S, Hiki N, Ohyama S, Aikou S, Sano T, Yamaguchi T. Outcome of surgical treatment for patients with locoregional recurrence of gastric cancer. Langenbecks Arch Surg. 2011. 396:161–166.22. National Research Council (U.S.). Committee to Assess Health Risks from Exposure to Low Level of Ionizing Radiation. Health risks from exposure to low levels of ionizing radiation: Beir vii phase 2. 2006. Washington, D.C.: National Academies Press.23. Alessio AM, Phillips GS. A pediatric ct dose and risk estimator. Pediatr Radiol. 2010. 40:1816–1821.24. Deak PD, Smal Y, Kalender WA. Multisection ct protocols: Sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology. 2010. 257:158–166.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Factors of Gastric Cancer and Lifestyle Modification for Prevention
- The Result of Conversion Surgery in Gastric Cancer Patients with Peritoneal Seeding
- Radiation Exposure from a Patient Treated with I-131 during Emergency Operation: A case report
- Gastric Complications after Adjuvant Radiotherapy for Breast Cancer
- Role of Adjuvant Radiotherapy in Gastric Cancer
