Korean J Gastroenterol.
2011 Mar;57(3):189-193. 10.4166/kjg.2011.57.3.189.
Q Fever as a Cause of Acute Hepatitis Accompanying Fever
- Affiliations
-
- 1Department of Internal Medicine, Korea University of Medical College, Seoul, Korea. kjhhepar@naver.com
- 2Department of Pathology, Korea University of Medical College, Seoul, Korea.
- KMID: 1128359
- DOI: http://doi.org/10.4166/kjg.2011.57.3.189
Abstract
- Q fever is a zoonotic infection caused by Coxiella burnetti, which has been previously regarded as an uncommon infectious disease in Korea but is sporadically reported recently. Common manifestations of acute Q fever usually present as influenza-like illness, pneumonia and occasionally hepatitis. Herein, we report 4 cases of acute Q fever as a cause of acute hepatitis and fever. All patients had fever and non-specific symptoms, and laboratory test showed acute hepatitis. Antibody surveys for many virus infections and bacterial cultures were negative. Finally, they were diagnosed acute Q fever by an indirect microimmunofluorescence test. Liver biopsy in 3 patients revealed granuloma including one with typical fibrin-ring. All patients had complete resolution of symptoms and signs with doxycycline treatment. Q fever should be considered in the differential diagnosis of patients with fever of unknown origin with acute hepatitis in Korea.
Keyword
MeSH Terms
Figure
-
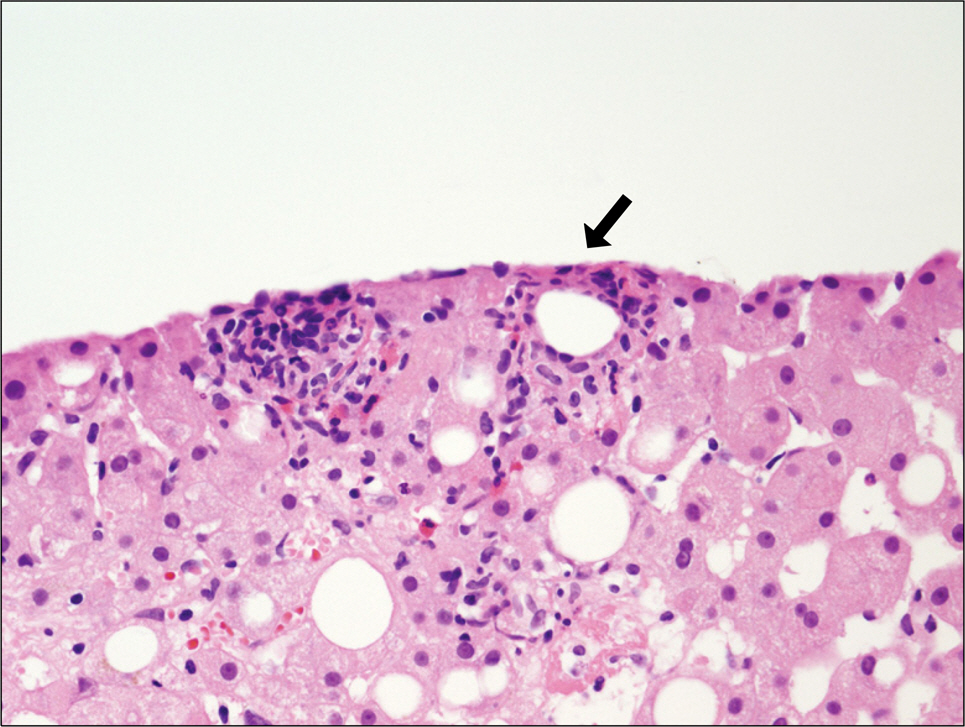
Fig. 1. A liver biosy specimen of case 1 (H&E stain, ×400). A lipid granuloma with a fibrinoid ring (arrow) within the inflammatory focus, and small vague granuloma were noted.
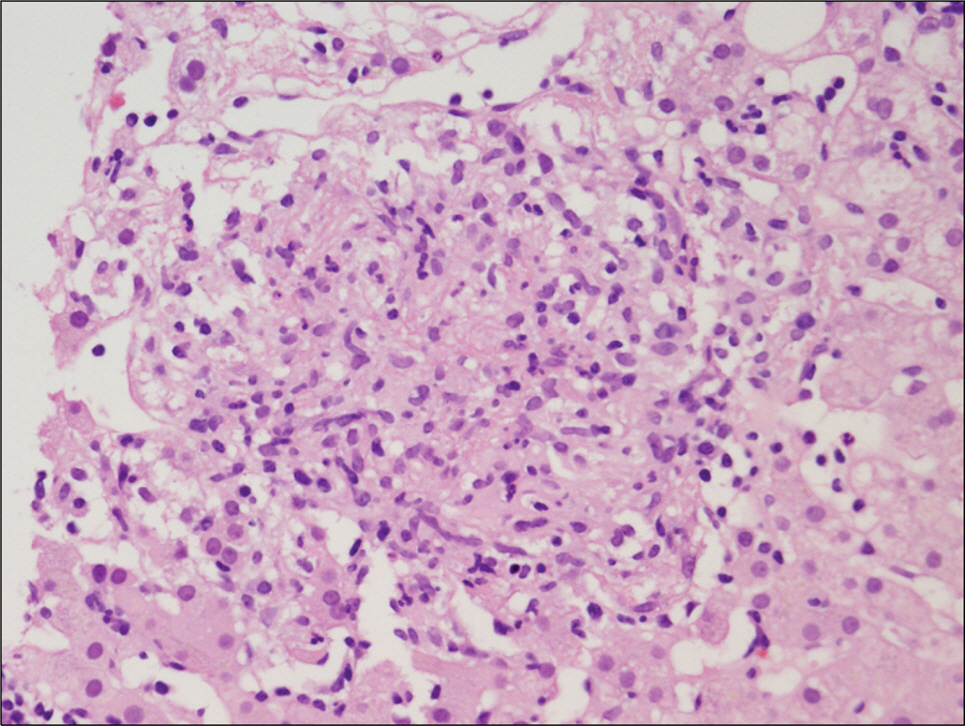
Fig. 2. A liver biosy specimen of case 2 (H&E stain, ×400). A granuloma composed of mixture of elongated epithelioid cells, histiocytes, and lymphocytes were noted.
Reference
-
References
1. Park HS, Lee EG, Lee SY, et al. A case of Q fever: associated with pancytopenia, hepatitis, and myocarditis. Korean J Infect Dis. 1992; 24:45–54.2. Parker NR, Barralet JH, Bell AM. Q fever. Lancet. 2006; 367:679–688.
Article3. Hartzell JD, Wood-Morris RN, Martinez LJ, Trotta RF. Q fever: epidemiology, diagnosis, and treatment. Mayo Clin Proc. 2008; 83:574–579.
Article4. Chang K, Yan JJ, Lee HC, Liu KH, Lee NY, Ko WC. Acute hepatitis with or without jaundice: a predominant presentation of acute Q fever in southern Taiwan. J Microbiol Immunol Infect. 2004; 37:103–108.5. Park YS, Lee KH, Park JY, Kim SK, Shin WS, Koh CM. Detection of antibodies to Coxiella burnetii antigen in the sera from resi-dents in Korea. J Korean Soc Microbiol. 1994; 29:333–339.6. Kim WJ, Hahn TW, Kim DY, et al. Seroprevalence of Coxiella burnetii infection in dairy cattle and non-symptomatic people for routine health screening in Korea. J Korean Med Sci. 2006; 21:823–826.7. Shin YJ, Yoo NC, Choi W, et al. A case pf Q fever. Korean J Intern Med. 1992; 42:690–698.8. Heo ST, Park MY, Choi YS, et al. Q fever as a cause of fever of unknown origin. Korean J Med. 2008; 74:100–105.9. Choi HC, Lee SH, Kim J, et al. A case of acute q Fever with severe acute cholestatic hepatitis. Gut Liver. 2009; 3:141–144.
Article10. Arricau-Bouvery N, Rodolakis A. Is Q fever an emerging or re-emerging zoonosis? Vet Res. 2005; 36:327–349.
Article11. Raoult D, Marrie T, Mege J. Natural history and pathophysiology of Q fever. Lancet Infect Dis. 2005; 5:219–226.
Article12. Ergas D, Keysari A, Edelstein V, Sthoeger ZM. Acute Q fever in Israel: clinical and laboratory study of 100 hospitalized patients. Isr Med Assoc J. 2006; 8:337–341.13. Lai CH, Chin C, Chung HC, et al. Acute Q fever hepatitis in patients with and without underlying hepatitis B or C virus infection. Clin Infect Dis. 2007; 45:e52–e59.
Article14. Crespo M, Sopeña B, Bordón J, de la Fuente J, Rubianes M, Martinez-Vázquez C. Steroids treatment of granulomatous hepatitis complicating Coxiella burnetii acute infection. Infection. 1999; 27:132–133.15. Srigley JR, Vellend H, Palmer N, et al. Q-fever. The liver and bone marrow pathology. Am J Surg Pathol. 1985; 9:752–758.16. Chung HJ, Chi HS, Cho YU, Jang S, Park CJ. Bone marrow fi-brin-ring granuloma: review of 24 cases. Korean J Lab Med. 2007; 27:182–187.
Article17. Fournier PE, Raoult D. Comparison of PCR and serology assays for early diagnosis of acute Q fever. J Clin Microbiol. 2003; 41:5094–5098.
Article18. Lever MS, Bewley KR, Dowsett B, Lloyd G. In vitro susceptibility of Coxiella burnetii to azithromycin, doxycycline, ciprofloxacin and a range of newer fluoroquinolones. Int J Antimicrob Agents. 2004; 24:194–196.19. Gikas A, Kofteridis DP, Manios A, Pediaditis J, Tselentis Y. Newer macrolides as empiric treatment for acute Q fever infection. Antimicrob Agents Chemother. 2001; 45:3644–3646.
Article20. Mandel GL, Bennet JE, Dolin R. Principles and practice of infectious diseases. 6th ed.Philadelphia: Elsevier Churchill Livingstone;2005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Q Fever with Severe Acute Cholestatic Hepatitis
- A case of acute pancreatitis and hepatitis associated with typhoid fever
- A Case of Typhoid Fever Complicated by Sensorineural Hearing Loss, Acute Pancreatitis and Hepatitis
- A Case of Icteric Typhoid Hepatitis Complicated with Splenic Infarction
- Multiple complications associated with hepatitis A in a pregnant woman
