Novel Influenza A (H1N1) Virus Infection in Children: Chest Radiographic and CT Evaluation
- Affiliations
-
- 1Department of Diagnostic Radiology, Dankook University College of Medicine, Dankook University Hospital, Chungnam 330-715, Korea. yslee@dkuh.co.kr
- 2Department of Pediatrics, Dankook University College of Medicine, Dankook University Hospital, Chungnam 330-715, Korea.
- KMID: 1119229
- DOI: http://doi.org/10.3348/kjr.2010.11.6.656
Abstract
OBJECTIVE
The purpose of this study was to evaluate the chest radiographic and CT findings of novel influenza A (H1N1) virus infection in children, the population that is more vulnerable to respiratory infection than adults.
MATERIALS AND METHODS
The study population comprised 410 children who were diagnosed with an H1N1 infection from August 24, 2009 to November 11, 2009 and underwent chest radiography at Dankook University Hospital in Korea. Six of these patients also underwent chest CT. The initial chest radiographs were classified as normal or abnormal. The abnormal chest radiographs and high resolution CT scans were assessed for the pattern and distribution of parenchymal lesions, and the presence of complications such as atelectasis, pleural effusion, and pneumomediastinum.
RESULTS
The initial chest radiograph was normal in 384 of 410 (94%) patients and abnormal in 26 of 410 (6%) patients. Parenchymal abnormalities seen on the initial chest radiographs included prominent peribronchial marking (25 of 26, 96%), consolidation (22 of 26, 85%), and ground-glass opacities without consolidation (2 of 26, 8%). The involvement was usually bilateral (19 of 26, 73%) with the lower lung zone predominance (22 of 26, 85%). Atelectasis was observed in 12 (46%) and pleural effusion in 11 (42%) patients. CT (n = 6) scans showed peribronchovascular interstitial thickening (n = 6), ground-glass opacities (n = 5), centrilobular nodules (n = 4), consolidation (n = 3), mediastinal lymph node enlargement (n = 5), pleural effusion (n = 3), and pneumomediastinum (n = 3).
CONCLUSION
Abnormal chest radiographs were uncommon in children with a swine-origin influenza A (H1N1) virus (S-OIV) infection. In children, H1N1 virus infection can be included in the differential diagnosis, when chest radiographs and CT scans show prominent peribronchial markings and ill-defined patchy consolidation with mediastinal lymph node enlargement, pleural effusion and pneumomediastinum.
Keyword
MeSH Terms
Figure
-
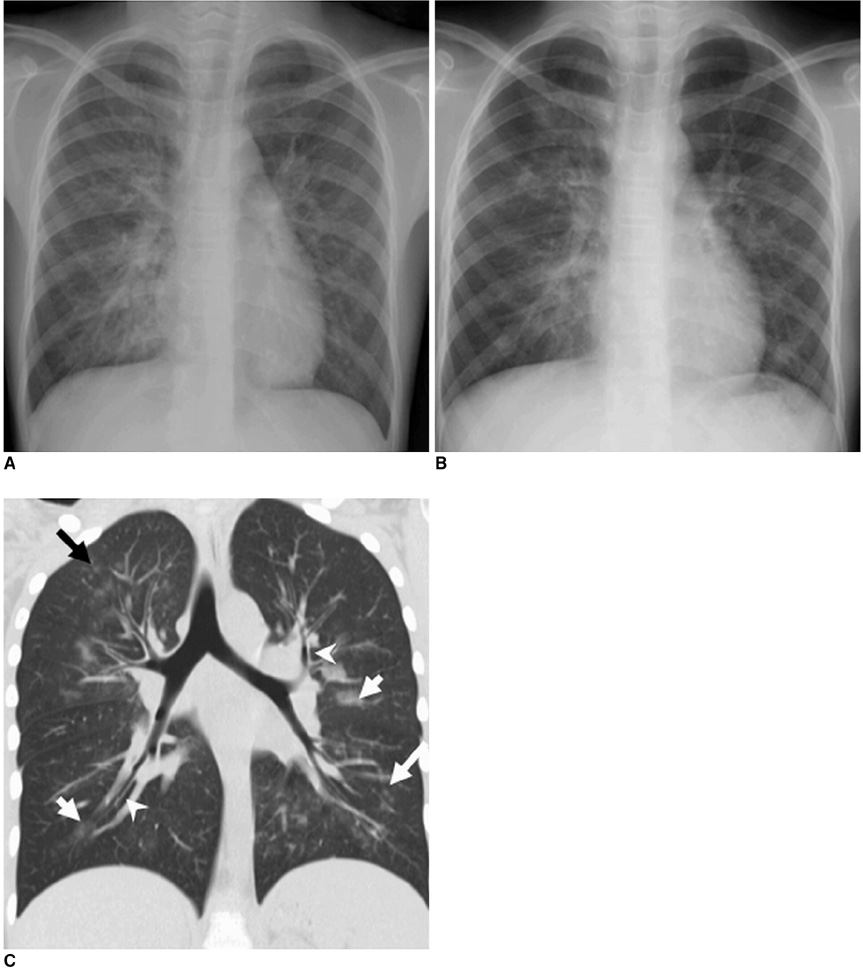
Fig. 1 9-year-old girl with laboratory-confirmed novel influenza A (H1N1). (Case No. 1) A. Initial chest radiograph shows consolidation in mainly right lower lung zone. Prominent peribronchial markings are also noted in right upper lung zone and left lung field. B. Chest radiograph four days later shows slightly improved consolidation in right lower lung zone. However, prominent peribronchial markings are still noted. C. Coronal CT scan five days after initial chest radiograph shows bilateral symmetric peribronchovascular interstitial thickening (arrowheads), centrilobular nodules (long arrows), and ground-glass opacities (short arrows).

Fig. 2 9-year-old boy with laboratory-confirmed novel influenza A (H1N1). A. Initial chest radiograph shows volume loss of right middle lobe. Prominent peribronchial markings are also noted in both lung fields. B. Chest radiograph three days later shows progression of atelectasis in right middle and lower lobes. C. Chest radiograph performed two days after radiograph in B shows improvement of atelectasis, but partial atelectasis of right middle lobe is still noted.

Fig. 3 6-year-old boy with laboratory-confirmed novel influenza A (H1N1). (Case No. 5) A. Initial chest radiograph shows consolidations in left upper and both middle lung zones. Prominent peribronchial markings are noted in right lung field. Pleural effusion (arrow) is also noted in left costophrenic angle. B. Coronal CT scan one day after initial chest radiograph shows bilateral peribronchial consolidations, which are predominant in left lung field.

Fig. 4 16-year-old boy with laboratory-confirmed novel influenza A (H1N1). (Case No. 2) A. Initial radiograph shows focal area of consolidation in left retrocardiac area. Prominent peribronchial markings are also seen in right lower lung zone and left lung fields. B. Magnified view of mediastinum on CT scan on same day shows several lymph nodes at right paratracheal and paraaortic nodal stations (arrows). C. High-resolution CT scan at level of left atrium shows pneumomediastinum (arrow) which was not seen on chest radiograph. D. High-resolution CT scan caudal to C shows ill-defined centrilobular nodules, ground-glass opacities (arrowhead), and focal area of consolidation (white arrow) mainly in left lower lobe. Pneumomediastinum (black arrow) is also noted.
Reference
-
1. Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009. 361:680–689.2. Neumann G, Noda T, Kawaoka Y. Emergence and pandemic potential of swine-origin H1N1 influenza virus. Nature. 2009. 459:931–939.3. Global alert and response: current WHO phase of pandemic alert? update58. World Health Organization Website. Accessed November 12, 2009. www.who.int/csr/disease/avian_influenza/phase/en/index.html.4. Centers for Disease Control and Prevention (CDC) Update: infectious with a swine-origin influenza A (H1N1) virus--United States and other countries, April 28, 2009. MMWR Morb Mortal Wkly Rep. 2009. 58:431–433.5. Update: Swine influenza A(H1N1) infections - California and Texas, April 2009. MMWR Morb Mortal Wkly Rep. 2009. 58:435–437.6. Yun BY, Kim MR, Park JY, Choi EH, Lee HJ, Yun CK. Viral etiology and epidemiology of acute lower respiratory tract infection in Korean children. Pediatr Infect Dis J. 1995. 14:1054–1059.7. Andronikou S. Pathological correlation of CT-detected mediastinal lymphadenopathy in children: the lack of size threshold criteria for abnormality. Pediatr Radiol. 2002. 32:912.8. Song HT, Park CK, Shin HJ, Choi YW, Jeon SC, Hahm CK, et al. Radiologic findings of childhood lower respiratory tract infection by influenza virus. J Korean Radiol Soc. 2002. 47:227–231.9. Kim EA, Lee KS, Primack SL, Yoon HK, Byun HS, Kim TS, et al. Viral pneumonias in adults: radiologic and pathologic findings. Radiographics. 2002. 22:S137–S149.10. Feldman PS, Cohan MA, Hierholzer WJ Jr. Fatal Hong Kong influenza: a clinical, microbiological and pathological analysis of nine cases. Yale J Biol Med. 1972. 45:49–63.11. Agarwal PP, Cinti S, Kazerooni EA. Chest radiographic and CT findings in novel swine-origin influenza A (H1N1) virus (S-OIV) infection. AJR Am J Roentgenol. 2009. 193:1488–1493.12. Lee EY, McAdam AJ, Chaudry G, Fishman MP, Zurakowski D, Boiselle PM. Swine-origin influenza A (H1N1) viral infection in children: initial chest radiographic findings. Radiology. 2010. 254:934–941.13. Oliveira EC, Marik PE, Colice G. Influenza pneumonia: a descriptive study. Chest. 2001. 119:1717–1723.14. Lee CW, Seo JB, Song JW, Lee HJ, Lee JS, Kim MY, et al. Pulmonary complication of novel influenza A (H1N1) infection: imaging features in two patients. Korean J Radiol. 2009. 10:531–534.15. Khater F, Moorman JP. Complications of influenza. South Med J. 2003. 96:740–743.16. Tanaka N, Matsumoto T, Kuramitsu T, Nakaki H, Ito K, Uchisako H, et al. High resolution CT findings in community-acquired pneumonia. J Comput Assist Tomogr. 1996. 20:600–608.17. Mollura DJ, Asnis DS, Crupi RS, Conetta R, Feigin DS, Bray M, et al. Imaging findings in a fatal case of pandemic swine-origin influenza A (H1N1). AJR Am J Roentgenol. 2009. 193:1500–1503.18. Ajlan AM, Quiney B, Nicolaou S, Müller NL. Swine-origin influenza A (H1N1) viral infection: radiographic and CT findings. AJR Am J Roentgenol. 2009. 193:1494–1499.19. Yun TJ, Kwon GJ, Oh MK, Woo SK, Park SH, Choi SH, et al. Radiological and clinical characteristics of a miliary outbreak of pandemic H1N1 2009 influenza virus infection. Korean J Radiol. 2010. 11:417–424.20. Zylak CM, Standen JR, Barnes GR, Zylak CJ. Pneumomediastinum revisited. Radiographics. 2000. 20:1043–1057.21. Damore DT, Dayan PS. Medical causes of pneumomediastinum in children. Clin Pediatr (Phila). 2001. 40:87–91.22. Abolnik I, Lossos IS, Breuer R. Spontaneous pneumomediastinum. A report of 25 cases. Chest. 1991. 100:93–95.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influenza Associated Pneumonia
- Chest Radiographic Findings of Novel Swine-Origin Influenza A (H1N1) Virus Infection in Children
- A Case of Novel Influenza A (H1N1) Virus Pneumonia Complicated Pnemomediastinum and Subcutenous Emphysema
- Radiologic Findings of Influenza A (H1N1) Pneumonia: Report of Two Cases
- RE: Pediatric Novel Influenza A (H1N1) Virus Infection: the Imaging Findings
