Superficial Endobronchial Lung Cancer: Radiologic-Pathologic Correlation
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Korea. kssong@amc.seoul.kr
- 2Department of Diagnostic Pathology, Asan Medical Center, University of Ulsan College of Medicine, Korea.
- KMID: 1118789
- DOI: http://doi.org/10.3348/kjr.2002.3.4.229
Abstract
OBJECTIVE
To analyze the plain chest radiographic and CT findings of superficial endobronchial lung cancer and to correlate these with the findings of histopathology. MATERIALS AND METHODS: This study involved 19 consecutive patients with pathologically proven lung cancer confined to the bronchial wall. Chest radiographs and CT scans were reviewed for the presence of parenchymal abnormalities, endobronchial nodules, bronchial obstruction, and bronchial wall thickening and stenosis. The CT and histopathologic findings were compared. RESULTS: Sixteen of the 19 patients had abnormal chest radiographic findings, while in 15 (79%), CT revealed bronchial abnormalities: an endobronchial nodule in seven, bronchial obstruction in five, and bronchial wall thickening and stenosis in three. Histopathologically, the lesions appeared as endobronchial nodules in 11 patients, irregular thickening of the bronchial wall in six, elevated mucosa in one, and carcinoma in situ in one. CONCLUSION: CT helps detect superficial endobronchial lung cancer in 79% of these patients, though there is some disagreement between the CT findings and the pathologic pattern of bronchial lesions. Although nonspecific, findings of bronchial obstruction or bronchial wall thickening and stenosis should not be overlooked, and if clinically necessary, bronchoscopy should be performed.
Keyword
MeSH Terms
Figure
-
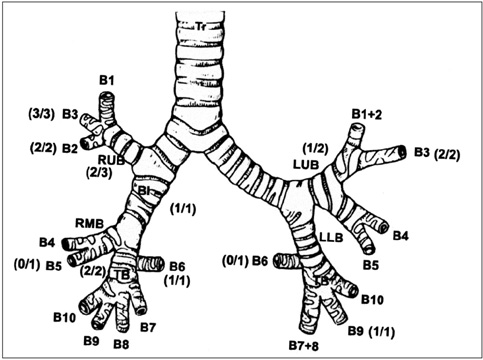
Fig. 1 Diagram showing the distribution of superficial endobronchial lung cancer according to its location. Numbers in parentheses indicate the number of endobronchial lesions identified at CT (the numerator) and the number of lesions histopathologically confirmed (the denominator).

Fig. 2 A 66-year-old man with chronic cough. A, B. Chest radiographs showing segmental consolidation in the superior segment of the right lower lobe. C. CT scans (10-mm-thick sections) demonstrate an endobronchial nodule at the distal bronchus intermedius (arrow) and consolidation in the superior segment of the right lower lobe. D. Photomicrography of pathologic specimen depicts an endobronchial nodule (arrows) and invasion of the full thickness of the bronchial wall (arrowhead) by the carcinoma (original magnification, ×100; hematoxylin-eosin staining).

Fig. 3 A 59-year-old man with blood-tinged sputum. A, B. Chest radiographs show segmental collapse in the anterior segment of the left upper lobe. C. CT scans (10-mm-thickness) depict bronchial obstruction and segmental atelectasis of the anterior segment of the left upper lobe. D. Photomicrography of pathologic specimen shows a polypoid mass in the anterior segmental bronchus of the left upper lobe (arrows), its invasive component extending through the full thickness of the bronchial wall (not shown here) (original magnification, ×400; hematoxylin-eosin staining).

Fig. 4 A 61-year-old man with blood-tinged sputum and weight loss. A. Chest radiograph reveals no abnormality. B. CT scan demonstrates patent right upper lobar bronchus with no endobronchial abnormality. C. Pathologic specimen depicts mucosal irregularity in the right upper lobar bronchus (arrows), and intramucosal invasion (arrowheads) (original magnification, ×40; hematoxylin-eosin staining).
Reference
-
1. Clifton FM. Revisions in the international system for staging lung cancer. Chest. 1997. 111:1710–1717.2. Carter D. Pathology of early squamous cell carcinoma of the lung. Pathol Annu. 1978. 13:131–147.3. Pearson FG, Thompson DW, Delarue NC. Experience with the cytologic detection, localization and treatment of radiographically undemonstrable bronchial carcinoma. J Thorac Cardiovasc Surg. 1967. 54:371–382.4. Martini N, Beattie EJ, Cliffton EE, Melamed MR. Radiologically occult lung cancer-report of 26 cases. Surg Clin N Am. 1974. 54:811–823.5. Woolner LB, David E, Fontana RS, et al. In-situ and early invasive bronchogenic carcinoma-report of 28 cases with postoperative survival data. J Thorac Cardiovasc Surg. 1970. 60:275–290.6. Potchen FJ, Bisesi MA. When is it malpractice to miss lung cancer on chest radiographics? Radiology. 1990. 175:29–32.7. Saida Y, Kujiraoka Y, Akaogi E, Ogata T, Kurosaki Y, Itai Y. Early squamous cell carcinoma of the lung: CT and pathologic correlation. Radiology. 1996. 201:61–65.8. Naidich DP, Zerhouni EA, Siegelman SS. Mediastinum. Computed tomography and magnetic resonance imaging of the thorax. 1999. 3rd ed. New York: Raven;38–150.9. Woolner LB, Fontana RS, Cortese DA, et al. Roentgenographically occult lung cancer: pathologic findings and frequency of multicentricity during a ten-year period. Mayo Clin Proc. 1984. 59:453–466.10. Fraser RS, Nester LM, Neil C, Pare PD. Pulmonary neoplasms In Fraser and Pare`s diagnosis of diseases of the chest. 1999. 4th ed. Philadelphia, Pennsylvania: Saunders Company;1070–1323.11. Charles SW, Benjamin MR, Andrew CM, John HA, Barbara HM, Zenon P. Primary carcinoma of the lung overlooked at CT: analysis of findings in 14 patients. Radiology. 1996. 199:109–115.12. Naidich DP, Zerhouni EA, Siegelman SS. Principles and techniques of thoracic CT and MR. Computed tomography and magnetic resonance imaging of the thorax. 1999. 3rd ed. New York: Raven;1–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Photodynamic Therapy for Endobronchial Obstruction due to Recurrent Lung Cancer : 2 Cases Report
- Synchronous Triple Primary Lung Cancer: A Rare Case with Radiologic-Pathologic Correlation
- Immunohistochemical Application to the Pathologic Diagnosis of Lung Cancer
- A Case of Endobronchial Fibroepithelial Polyp
- Endobronchial IVletastasis of Parosteal Osteosarcoma: A Case Report
