A Spinal Cord Astrocytoma and Its Concurrent Osteoblastic Metastases at the Time of the Initial Diagnosis: a Case Report and Literature Review
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiological Science, Gangnam Severance Hospital, Yonsei University, Seoul 135-720, Korea. agn70@yuhs.ac
- 2Department of Pathology, Gangnam Severance Hospital, Yonsei University, Seoul 135-720, Korea.
- 3Department of Nuclear Medicine, Gangnam Severance Hospital, Yonsei University, Seoul 135-720, Korea.
- 4Department of Neurosurgery, the Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University, Seoul 135-720, Korea.
- 5Department of Orthopedic Surgery, Gangnam Severance Hospital, Yonsei University, Seoul 135-720, Korea.
- KMID: 1116448
- DOI: http://doi.org/10.3348/kjr.2011.12.5.620
Abstract
- Bone metastasis from a spinal cord astrocytoma has been reported only twice in the English medical literature. It is generally known that bone metastasis is found after the initial diagnosis with/without intervening surgery rather than being found at the time of the diagnosis of astrocytoma. The purpose of this article is to report for the first time a case of concurrent bone metastasis from a spinal cord astrocytoma at the time of diagnosing the spinal cord astrocytoma.
Keyword
MeSH Terms
Figure
-
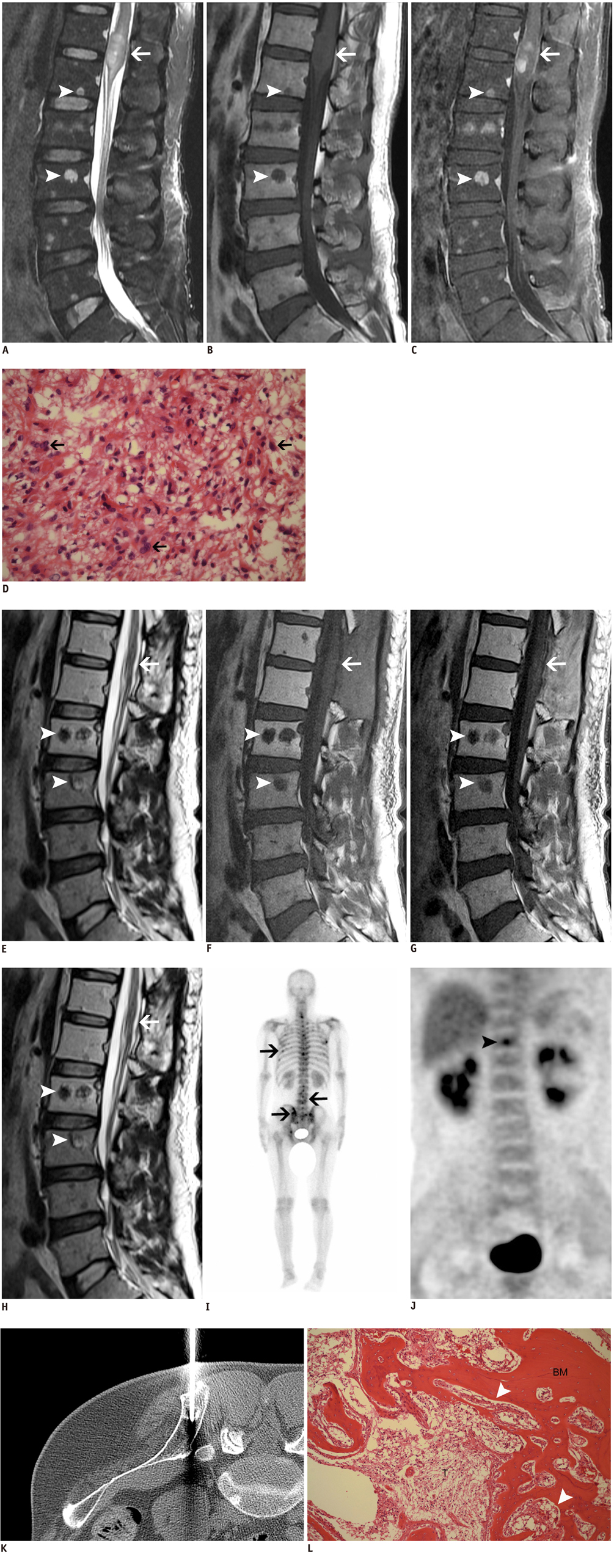
Fig. 1 Bone metastasis identified concurrently with primary spinal cord astrocytoma. A-C. Fat suppressed T2-weighted image shows heterogeneous hyperintense mass of spinal cord (arrows) at level of T12 and L1 vertebrae (A), T1-weighted image shows isointensity of this mass (B), and fat-suppressed contrast enhanced T1-weighted image shows multifocal nodular enhancement (C). Fat suppressed T2-weighted image shows heterogeneous hyperintense multiple metastatic bone marrow lesions (arrowheads) (A), T1-weighted image shows hypointensity of these lesions (B) and fat suppressed contrast enhanced T1-weighted image shows heterogeneous enhancement (C). D. Microscopic examination (Hematoxylin & Eosin staining, original magnification: × 400) reveals high cellularity and nuclear pleomorphism (arrows) in fibrillary background without microvessel proliferation or tumor necrosis, which all suggests anaplastic astrocytoma. E-H. T2-weighted image shows aggravated multiple bone marrow lesions (arrowheads) with variable signal intensity (E), T1-weighted image shows hypointensity of these lesions (F) and contrast enhanced T1-weighted image shows variable contrast enhancement (G). These lesions, which correspond to those of MR images, are depicted as osteoblastic lesions on sagittal reformatted CT images of spine (H). I, J. Scintigraphy (I) and whole body 18F-FDG PET-CT (J) images of patient. Whole body bone scan (I) shows multiple foci of heterogeneously increased bony uptake (arrows) at thoracolumbar spine, rib cage and pelvic bones, which are thought to be consistent with multiple bony lesions seen on CT and MRI. Whole body FDG PET image (J) shows increased focal FDG uptake (arrowhead) of vertebral body, which is clearly visualized as being located in T11 vertebral body on fusion image of PET-CT. Extraskeletal FDG uptake is not observed. K, L. CT-guided localization using guide pin for subsequent open bone biopsy (K) and photomicrograph of surgical specimen from excised bone (L). CT image obtained with localization clearly shows guide pin whose tip is located at center of iliac bone, which contains osteoblastic lesions (K). Histologic examination of specimen (Hematoxylin & Eosin staining, original magnification × 100) reveals bone marrow and metastatic tumor (T). Bone marrow (BM) is infiltrated by metastatic tumor cells (arrowheads) that show histologic findings identical to those of spinal cord tumor.
Reference
-
1. Roonprapunt C, Houten JK. Spinal cord astrocytomas: presentation, management, and outcome. Neurosurg Clin N Am. 2006. 17:29–36.2. Newman RP, Schaefer EJ, Thomas CB, Oldfield EH. Abetalipoproteinemia and metastatic spinal cord glioblastoma. Arch Neurol. 1984. 41:554–556.3. Eade OE, Urich H. Metastasising gliomas in young subjects. J Pathol. 1971. 103:245–256.4. Fabi A, Vidiri A, Carapella C, Pace A, Occhipinti E, Caroli F, et al. Bone metastasis from glioblastoma multiforme without central nervous system relapse: a case report. Anticancer Res. 2004. 24:2563–2565.5. Beauchesne P, Soler C, Mosnier JF. Diffuse vertebral body metastasis from a glioblastoma multiforme: a technetium-99m Sestamibi single-photon emission computerized tomography study. J Neurosurg. 2000. 93:887–890.6. Rajagopalan V, El Kamar FG, Thayaparan R, Grossbard ML. Bone marrow metastases from glioblastoma multiforme--A case report and review of the literature. J Neurooncol. 2005. 72:157–161.7. Utsuki S, Tanaka S, Oka H, Iwamoto K, Sagiuchi T, Fujii K. Glioblastoma multiforme metastasis to the axis. Case report. J Neurosurg. 2005. 102:540–542.8. Mihara F, Ikeda M, Rothman MI, Numaguchi Y, Kristt D. Vertebral body metastasis of glioblastoma multiforme with epidural mass formation. Contrast-enhanced MRI study. Clin Imaging. 1994. 18:386–389.9. Myers T, Egelhoff J, Myers M. Glioblastoma multiforme presenting as osteoblastic metastatic disease: case report and review of the literature. AJNR Am J Neuroradiol. 1990. 11:802–803.10. Taoka T, Mayr NA, Lee HJ, Yuh WT, Simonson TM, Rezai K, et al. Factors influencing visualization of vertebral metastases on MR imaging versus bone scintigraphy. AJR Am J Roentgenol. 2001. 176:1525–1530.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intramedullary Spinal Cord Astrocytoma Associated with Neurofibromatosis Type 1
- A Case of Spinal Cord Astrocytoma Associated with Hemorrhage
- Intracranial Dissemination from Spinal Cord Anaplastic Astrocytoma
- Intramedullary Spinal Cord Metastasis: A Report of Two Cases and a Review of the Literature
- Intracranial Metastases of Cervical Intramedullary Low-Grade Astrocytoma without Malignant Transformation in Adult
