Korean J Ophthalmol.
2004 Jun;18(1):29-34. 10.3341/kjo.2004.18.1.29.
The Efficacy of Multi-Zone Cross-Cylinder Method for Astigmatism Correction
- Affiliations
-
- 1Department of Ophthalmology, Seoul Adventist Hospital, Seoul, Korea.
- KMID: 1115780
- DOI: http://doi.org/10.3341/kjo.2004.18.1.29
Abstract
- The purpose of this study is to assess the efficacy of the multi-zone cross-cylinder method as compared with the single method for astigmatism correction using LASIK. This prospective study enrolled 40 patients (52 eyes) who underwent the cross-cylinder method using LASIK, and 52 patients (60 eyes) who underwent the single method using LASIK: all patients were given a diagnosis of complex myopic astigmatism from the department of ophthalmology of this hospital between January 2002 and July 2003. Preoperatively, the mean spherical equivalent refraction was .3.85 +/- 1.13 D in the cross-cylinder group and .4.05 +/-1.20 D in the single method group (p = 0.23). The mean cylinder was .2.05 +/-1.58 D in the cross-cylinder group and .1.95 +/-1.12 D in the single method group (p = 0.31). 6 months after treatment the results were a mean spherical equivalent refraction of .0.26 +/-0.30 D in the crosscylinder group and -0.34 +/-0.35 D in the single method group (p = 0.13). The mean cylinder was .0.38 +/-0.29 D in the cross-cylinder group and .0.45 +/-0.30 D in the single method group (p = 0.096). There were no statistically significant differences between the two groups. The mean BCVA was not different from mean preoperative BCVA in both groups (i.e., 0.98 +/-0.10, 0.96 +/-0.25, p = 0.86). Postoperatively, patient complications that included night halo, glare and corneal haze were not noted in either group. In conclusion, the results of cross-cylinder method are no different from the single method for the correction of a complex astigmatism. In the future, studies will have to be conducted to assess the efficacy of the cross-cylinder method in consideration of those factors that can affect the postoperative outcome.
Keyword
MeSH Terms
Figure
-
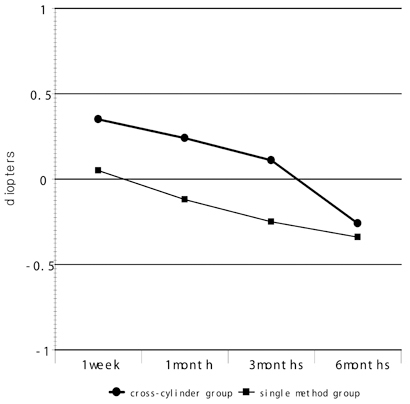
Fig. 1 The graph of postoperative mean spherical equivalent changes (D) in 6 months after cross-cylinder ablation.
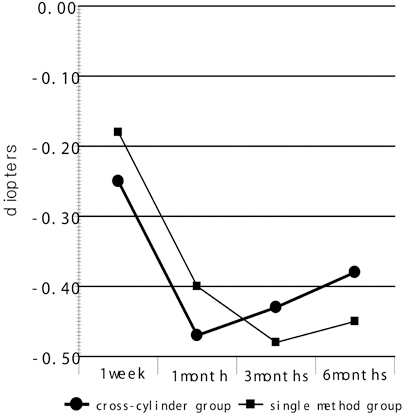
Fig. 2 The graph of postoperative mean cylinderic changes (D) in 6 months after cross-cylinder ablation.
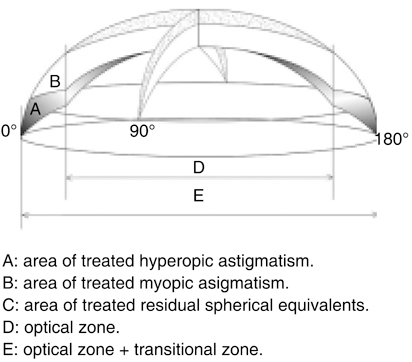
Fig. 3 Myopic with-the-rule astigmatism corrected with a cross-cylinder method. The surgical strategy involved ablating half the amount of the cylinder along steepest meridian, the other half in a subsequent step along the flattest meridian; thereafter, the spherical equivalent was corrected.
Reference
-
1. Pallikaris IG, Papatzanaki ME, Stathi EZ. Laser in situ keratomileusis. Lasers Surg Med. 1990. 10:463–468.2. Hersh PS, Abbassi R. Summit PRK-LASIK Study Group. Surgically induced astigmatism after photorefractive keratectomy and laser in situ keratomileusis. J Cataract Refract Surg. 1999. 25:389–398.3. Dulaney DD, Barnet RW, Perkins SA, Kezirian GM. Laser in situ keratomileusis for myopia and astigmatism: 6 month results. J Cataract Refract Surg. 1998. 24:758–764.4. Vinciguerra P, Sborgia M, Epstein D, Azzolini M, MacRae S. Photorefractive keratectomy to correct myopic or hyperopic astigmatism with a cross-cylinder ablation. J Refract Surg. 1999. 15:S183–S185.5. Sohn JH, Cha HW, Kim YJ. Excimer laser photorefractive keratectomy-multicenter study. J Korean Ophthalmol Soc. 1993. 34:1208–1212.6. Jun SG, Cha HW, Kim YJ. Excimer laser photorefractive keratectomy: two-year follow-up. J Korean Ophthalmol Soc. 1997. 38:17–26.7. Pallikaris IG, Siganos DS. Excimer laser in situ keratomileusis and photorefractive keratectomy for correction of high myopia. J Refract Corneal Surg. 1994. 10:498–510.8. Guell JL, Muller A. Laser in situ keratomileusis (LASIK) for myopia from -7 to -18 diopters. J Refract Surg. 1996. 12:222–228.9. Huang D, Stulting RD, Carr JD, Thompson KP. Multiple regression and vector analyses of laser in situ keratomileusis for myopia and astigmatism. J Refract Surg. 1999. 15:538–549.10. Vinciguerra P, Camesasca FI. Cross-cylinder ablation. Customized Corneal Ablation. The Quest for SuperVision. 2001. 28. SLACK Incorporated;325–326.11. Salchow DJ, Zirm ME, Stieldorf C, Parisi A. Laser in situ keratomileusis for myopia and myopic astigmatism. J Cataract Refract Surg. 1998. 24:175–182.12. Salah T, Waring GO III, Magharby AE, Moadel K, Grimm SB. Excimer Laser in situ Keratomileusis under a corneal flap for myopia of 2 to 20 diopters. Am J Ophthalmol. 1996. 121:143–155.13. Choi YK, Suh Y, Joo CK. Myopic regression and its mechanism after LASIK surgery. J Korean Ophthalmol Soc. 2000. 41:620–626.14. Fraenkel GE, Webber SK, Sutton GL. Toric laser in situ keratomileusis for myopic astigmatism using an ablatable mask. J Refract Surg. 1999. 15:111–117.15. Zaldivar R, Davidorf JM, Oscherow S. Laser in situ keratomileusis for myopia from -5.50 to -11.50 diopters with astigmatism. J Refract Surg. 1998. 14:19–25.16. Kim SJ, Lee YJ, Cha HW. Astigmatic correction of LASIK. J Korean Ophthalmol Soc. 2001. 42:967–971.17. Hersh PS, Shah SI, Geiger D, Holladay JT. Corneal optical irregularity after excimer laser photorefractive keratectomy. The Summit Photorefractive Keratectomy Topography Study Group. J Cataract Refract Surg. 1996. 22:197–204.
