Yonsei Med J.
2009 Oct;50(5):725-728. 10.3349/ymj.2009.50.5.725.
Successful Treatment of Syncope with Chemotherapy Irresponsive to Cardiac Pacemaker in Head and Neck Cancer
- Affiliations
-
- 1Department of Internal Medicine, Post-Graduate Medical School, Gyeongsang National University, Jinju, Korea. newatp@gnu.ac.kr
- 2Department of Otolaryngology, Post-Graduate Medical School, Gyeongsang National University, Jinju, Korea.
- 3Gyeongsang Institute of Health Science, Jinju, Korea.
- 4Gyeongnam Regional Cencer Center, Jinju, Korea.
- KMID: 1103831
- DOI: http://doi.org/10.3349/ymj.2009.50.5.725
Abstract
- Recurrent syncope as a complication of recurrent neck malignancy is an uncommon but well documented association. The syncope is presumed to occur when a tumor mass invades the baroreceptor within the carotid sinus or when it disrupts the afferent nerve fibers of the glossopharyngeal nerve. A 59-year-old man presented with recurrent syncope and headache. He had a wide local excision including tonsillectomy and modified left radical neck dissection for tonsilar cancer 4 years ago. A computed tomography scan revealed ill-defined lesions in left parapharyngeal, carotid space and right upper jugular region. After clinical evaluation, cardiac pacemaker was placed, but he still suffered from the syncope. Then, he received the chemotherapy with docetaxel and cisplatin. The last hypotension event occurred on day 10 of the chemotherapy. Six months after 3 cycles of chemotherapy, he remained in complete remission and resolution of syncope. We report a case in which syncope was associated with a recurrence of tonsilar cancer and successfully treated with chemotherapy.
Keyword
MeSH Terms
-
Antineoplastic Combined Chemotherapy Protocols/*therapeutic use
Carcinoma, Squamous Cell/*complications/drug therapy/radiography
Cisplatin/*therapeutic use
Head and Neck Neoplasms/*complications/drug therapy/radiography
Humans
Male
Middle Aged
Neoplasm Recurrence, Local/*complications/drug therapy
*Pacemaker, Artificial
Syncope/*drug therapy/etiology
Taxoids/*therapeutic use
Tonsillar Neoplasms/*complications/drug therapy/radiography
Figure
-
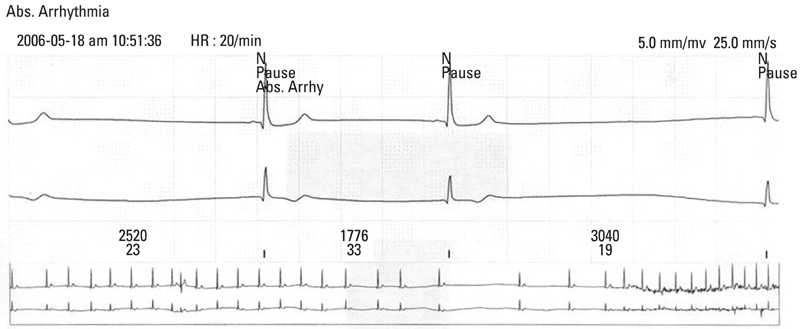
Fig. 1 A 24 hr Holter monitoring showed long sinus pauses for up to 3 seconds.

Fig. 2 A computed tomography scan revealed ovoid mass lesion compressing the left internal carotid artery.

Fig. 3 A computed tomography scan performed after 3 cycles of chemotherapy showed a considerable reduction of the mass which compresses the left internal carotid artery.
Reference
-
1. Macdonald DR, Strong E, Nielsen S, Posner JB. Syncope from head and neck cancer. J Neurooncol. 1983. 1:257–267.2. Lin RH, Teng MM, Wang SJ, Yeh TP, Liao KK, Liu HC. Syncope as the presenting symptom of nasopharyngeal carcinoma. Clin Neurol Neurosurg. 1994. 96:152–155.3. Chen-Scarabelli C, Kaza AR, Scarabelli T. Syncope due to nasopharyngeal carcinoma. Lancet Oncol. 2005. 6:347–349.
Article4. Bauer CA, Redleaf MI, Gartlan MG, Tsue TT, McColloch TM. Carotid sinus syncope in head and neck cancer. Laryngoscope. 1994. 104:497–503.
Article5. Choi YM, Mafee MF, Feldman LE. Successful treatment of syncope in head and neck cancer with induction chemotherapy. J Clin Oncol. 2006. 24:5332–5333.
Article6. Hong AM, Pressley L, Stevens GN. Carotid sinus syndrome secondary to head and neck malignancy: case report and literature review. Clin Oncol (R Coll Radiol). 2000. 12:409–412.
Article7. Hawkins J, Lewis HD, Emmot W, Vacek JL. Vasodepressive carotid sinus hypersensitivity with head and neck malignancy: treatment with propranolol. Am Heart J. 1991. 122:234–235.8. Sutherland JA, Stobie P, Swarup V, Tierney SP, Lin AC, Burke MC. Hypersensitive carotid sinus syndrome due to neurofibromatosis-1 and manifested by repeated episodes of syncope. Pacing Clin Electrophysiol. 2004. 27:1571–1573.
Article9. Venkatraman V, Lee L, Nagarajan DV. Lymphoma and malignant vasovagal syndrome. Br J Haematol. 2005. 130:323.
Article10. Worth PF, Stevens JC, Lasri F, Brew S, Reilly MM, Mathias CJ, Rudge P. Syncope associated with pain as the presenting feature of neck malignancy: failure of cardiac pacemaker to prevent attacks in two cases. J Neurol Neurosurg Psychiatry. 2005. 76:1301–1303.
Article11. Weiss S, Baker JR. The carotid sinus reflex in health and disease: its role in the causation of fainting and convulsions. Medicine. 1933. 12:297–354.12. McIntosh SJ, Lawson J, Bexton RS, Gold RG, Tynan MM, Kenny RA. A study comparing VVI and DDI pacing in elderly patients with carotid sinus syndrome. Heart. 1997. 77:553–557.
Article13. Walter PF, Crawley IS, Dorney ER. Carotid sinus hypersensitivity and syncope. Am J Cardiol. 1978. 42:396–403.
Article14. Johnston RT, Redding VJ. Glossopharyngeal neuralgia associated with cardiac syncope: long term treatment with permanent pacing and carbamazepine. Br Heart J. 1990. 64:403–405.
Article15. Chen-Scarabelli C, Scarabelli TM. Neurocardiogenic syncope. BMJ. 2004. 329:336–341.
Article16. Thomas JE. Hyperactive carotid sinus reflex and carotid sinus syncope. Mayo Clin Proc. 1969. 44:127–139.17. Dykman TR, Montgomery EB Jr, Gerstenberger PD, Zeiger HE, Clutter WE, Cryer PE. Glossopharyngeal neuralgia with syncope secondary to tumor. Treatment and pathophysiology. Am J Med. 1981. 71:165–170.18. Dreyfuss AI, Clark JR, Norris CM, Rossi RM, Lucarini JW, Busse PM, et al. Docetaxel: an active drug for squamous cell carcinoma of the head and neck. J Clin Oncol. 1996. 14:1672–1678.
Article19. Guntinas-Lichius O, Appenrodt S, Veelken F, Krug B. Phase II study of weekly docetaxel and cisplatin in patients with advanced recurrent and metastatic head and neck cancer. Laryngoscope. 2006. 116:613–618.
Article20. Browman GP, Cronin L. Standard chemotherapy in squamous cell head and neck cancer: what we have learned from randomized trials. Semin Oncol. 1994. 21:311–319.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Permanent cardiac pacemaker therapy in a patient with swallow syncope
- Cardiogenic Dizziness Treated with Cardiac Pacemaker: Reports of Four Cases
- Severe Pain Attack Associated with Neurocardiogenic Syncope Induced by Glossopharyngeal Neuralgia: Successful Treatment with Carbamazepine and a Permanent Pacemaker: A Case Report
- Permanent Pacemaker Implantation in a Patient with Cardiac Syncope Associated with Glossopharyngeal Neuralgia
- Radiotherapy of Patient with Implanted Cardiac Pacemaker
