Depiction of Viable Tumor in Hepatocellular Carcinoma Treated with Transarterial Chemoembolization: Multiphasic Helical CT with Review of the Previous Serial CT Images
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea. dichoi@smc.samsung.co.kr
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- KMID: 1102711
- DOI: http://doi.org/10.3348/kjr.2005.6.3.153
Abstract
OBJECTIVE
The purpose of our study was to assess whether a review of multiphasic helical CT combined with the previous serial CT images could be helpful to depict a viable tumor in hepatocellular carcinoma treated with transarterial chemoembolization. MATERIALS AND METHODS: Twenty-four consecutive patients with 35 hepatocellular carcinomas underwent transarterial chemoembolization followed by hepatic resection. First, three radiologists independently analyzed the last CT images taken before resection for the presence of viable tumor. A second analysis was then performed using the last CT combined with the previous serial CT images. The CT analyses were then compared with the pathologic results. The added value of the review of the previous serial CT images was evaluated by performing a receiver operating characteristic analysis. The sensitivity, specificity and diagnostic accuracy for the depiction of viable tumor were also assessed, and the characteristics of the false-negative lesions were pathologically evaluated. RESULTS: The mean diagnostic accuracies (Az values) for the depiction of viable tumor with using the last CT alone and with the review of the previous serial CT images for all observers were 0.885 and 0.901, respectively, which were not significantly difference (p> 0.05). However, the additional review of the previous serial CT images allowed the observers to render a correct diagnosis for three lesions that had been incorrectly diagnosed with the review of last CT alone. The sensitivity, specificity and diagnostic accuracy of the last CT along with the review of the previous serial CT images were 78%, 97% and 84%, respectively. All of the 16 false-negative lesions diagnosed by each observer showed 90% or greater necrosis on the pathologic examination. CONCLUSION: For the depiction of viable tumor in hepatocellular carcinoma treated with transarterial chemoembolization, although the difference in the diagnostic accuracies was not statistically significant, a review of the multiphasic helical CT combined with the previous serial CT images could help reach a correct diagnosis for those lesions incorrectly diagnosed with the review of the last CT alone.
Keyword
MeSH Terms
-
Tomography, X-Ray Computed
*Tomography, Spiral Computed
Tissue Survival
Sensitivity and Specificity
Neoplasm, Residual/*radiography
Middle Aged
Male
Liver Neoplasms/*radiography/*therapy
Humans
Hepatectomy
Female
False Negative Reactions
*Chemoembolization, Therapeutic
Carcinoma, Hepatocellular/*radiography/*therapy
Aged
Adult
Figure
-
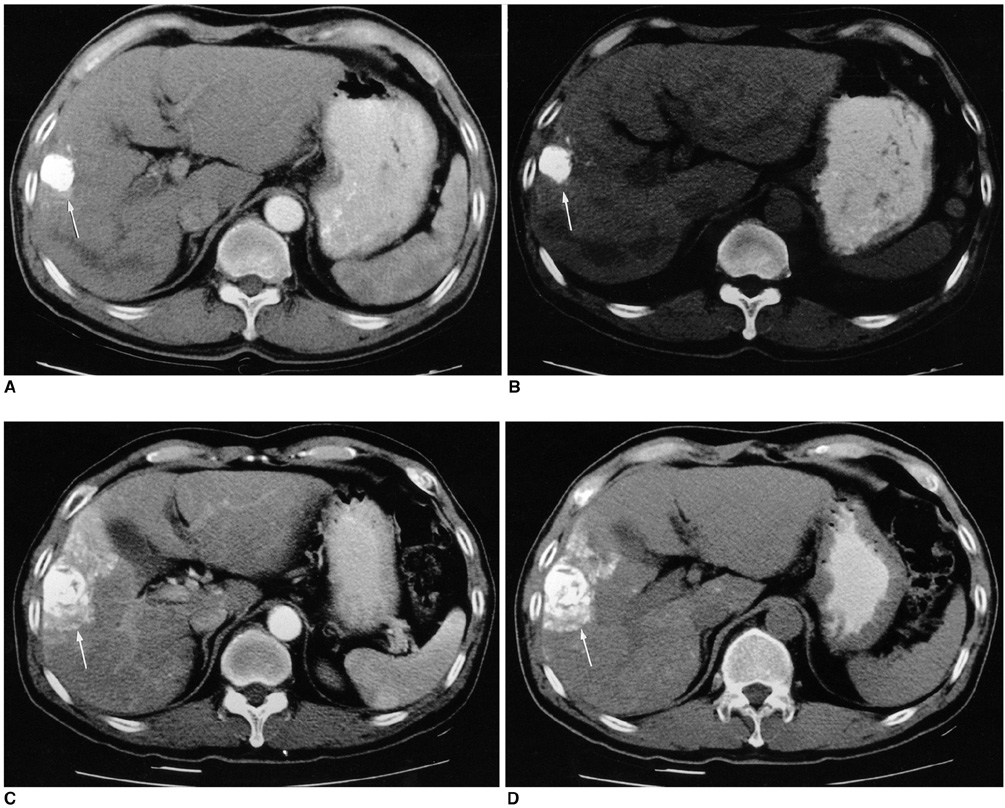
Fig. 1 A 56-year-old man who had undergone one time preoperative treatment with transarterial chemoembolization and right lobectomy. The pathologic examination revealed totally necrotic tumor. A, B. On the last contrast-enhanced CT, the lesion that is a focal slightly hyperattenuating area (arrow) adjacent to the iodized oil-containing nodule on the hepatic arterial phase CT image (A) appears as an isoattenuating area (arrow) at the corresponding region on the unenhanced CT image (B). This lesion was interpreted as a viable tumor by all the observers after reviewing the last CT alone. C, D. On the second to the last CT taken three weeks after the transarterial chemoembolization, the hepatic arterial phase (C) and unenhanced CT images (D) show that the hyperattenuating lesion seen in Figure A appears to be iodized oil-containing hepatic parenchyma (arrow). After reviewing the previous serial CT images, the two observers interpreted this hyperattenuating lesion on the last hepatic arterial phase CT as an arteriovenous shunt, and they changed the confidence level to probably not viable tumor.

Fig. 2 A 52-year-old man who had undergone three transarterial chemoembolization treatments and right hepatic lobectomy. A, B. The unenhanced CT images show two compact iodized oil-containing nodules at S8 (arrow) and S6 (arrowhead) of the liver. C-F. These contrast-enhanced CT scans obtained during the arterial phase (C, D) and the delayed phase (E, F) show neither enhancing portions nor defects within the iodized oil-containing nodules at S8 (arrow) and S6 (arrowhead). The two tumors were interpreted as non-viable tumors by all the observers. The pathologic examination revealed that the S6 tumor was 90% necrotic and that the S8 tumor was totally necrotic.
Reference
-
1. Lim JH, Choi D, Kim SH, Lee SJ, Lee WJ, Lim HK, et al. Detection of hepatocellular carcinoma: value of adding delayed phase imaging to dual-phase helical CT. AJR Am J Roentgenol. 2002. 179:67–73.2. Hwang GJ, Kim MJ, Yoo HS, Lee JT. Nodular hepatocellular carcinomas: detection with arterial-, portal-, and delayed-phase images at spiral CT. Radiology. 1997. 202:383–388.3. Choi BI, Lee KH, Han JK, Lee JM. Hepatic arterioportal shunts: dynamic CT and MR features. Korean J Radiol. 2002. 3:1–15.4. Kim HC, Kim AY, Han JK, Chung JW, Lee JY, Park JH, et al. Hepatic arterial and portal venous phase helical CT in patients treated with transcatheter arterial chemoembolization for hepatocellular carcinoma: added value of unenhanced images. Radiology. 2002. 225:773–780.5. Fleiss JL. Fleiss JL, editor. The measurement of interrater agreement. Statistical methods for rates and proportions. 1981. 2nd ed. New York, NY: John Wiley & Sons;212–236.6. World Health Organization. WHO handbook of reporting results of cancer treatment. 1979. Geneva: World Health Organization;WHO offset publication No. 48.7. Choi BI, Kim HC, Han JK, Park JH, Kim YI, Kim ST, et al. Therapeutic effect of transcatheter oily chemoembolization therapy for encapsulated nodular hepatocellular carcinoma: CT and pathologic findings. Radiology. 1992. 182:709–713.8. Takayasu K, Arii S, Matsuo N, Yoshikawa M, Ryu M, Takasaki K, et al. Comparison of CT findings with resected specimens after chemoembolization with iodized oil for hepatocellular carcinoma. AJR Am J Roentgenol. 2000. 175:699–704.9. Lee JK, Chung YH, Song BC, Shin JW, Choi WB, Yang SH, et al. Recurrences of hepatocellular carcinoma following initial remission by transcatheter arterial chemoembolization. J Gastroenterol Hepatol. 2002. 17:52–58.10. Bonaldi VM, Bret PM, Reinhold C, Arti M. Helical CT of the liver: value of an early arterial phase. Radiology. 1995. 197:357–363.11. Baron RL, Oliver JH III, Dodd GD III, Nalesnik M, Holbert BL, Carret B. Hepatocellular carcinoma: evaluation with biphasic, contrast-enhanced, helical CT. Radiology. 1996. 199:505–511.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Metastatic Adrenal Tumor from a Hepatocellular Carcinoma: Combination Therapy with Transarterial Chemoembolization and Radiofrequency Ablation
- Intraductal migration of necrotic hepatocellular carcinoma: A possible cause of obstructive cholangitis after chemoembolization
- A Case of Infiltrative Hepatocellular Carcinoma with Main Portal Vein Tumor Thrombosis Successfully Treated by Transarterial Chemoembolization
- Prediction of Complete Necrosis of Hepatocellular Carcinoma Treated with Transarterial Chemoembolization Prior to Liver Transplantation
- Complications Related to Transarterial Treatment of Hepatocellular Carcinoma: A Comprehensive Review
