Imaging Findings of Intrahepatic Bile Duct Adenoma (Peribiliary Gland Hamartoma): a Case Report and Literature Review
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 137-701, Korea. serha@catholic.ac.kr
- 2Department of Pathology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 137-701, Korea.
- 3Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 137-701, Korea.
- KMID: 1102582
- DOI: http://doi.org/10.3348/kjr.2010.11.5.560
Abstract
- Intrahepatic bile duct adenoma is a rare benign epithelial hepatic tumor derived from bile duct cells. We report the imaging findings of a patient with bile duct adenoma, which appeared as a small heterogeneously enhancing mass with focal small cystic change on CT and MRI. Follow-up images at seven months showed a slight increase in tumor size, which could be partly explained by intratumoral hemorrhage on pathologic examination. Although rare, bile duct adenoma should be considered as a differential diagnosis of a small hypervascular tumor located in the periphery of liver. Focal cystic change and intratumoral hemorrhage may occur.
MeSH Terms
Figure
-
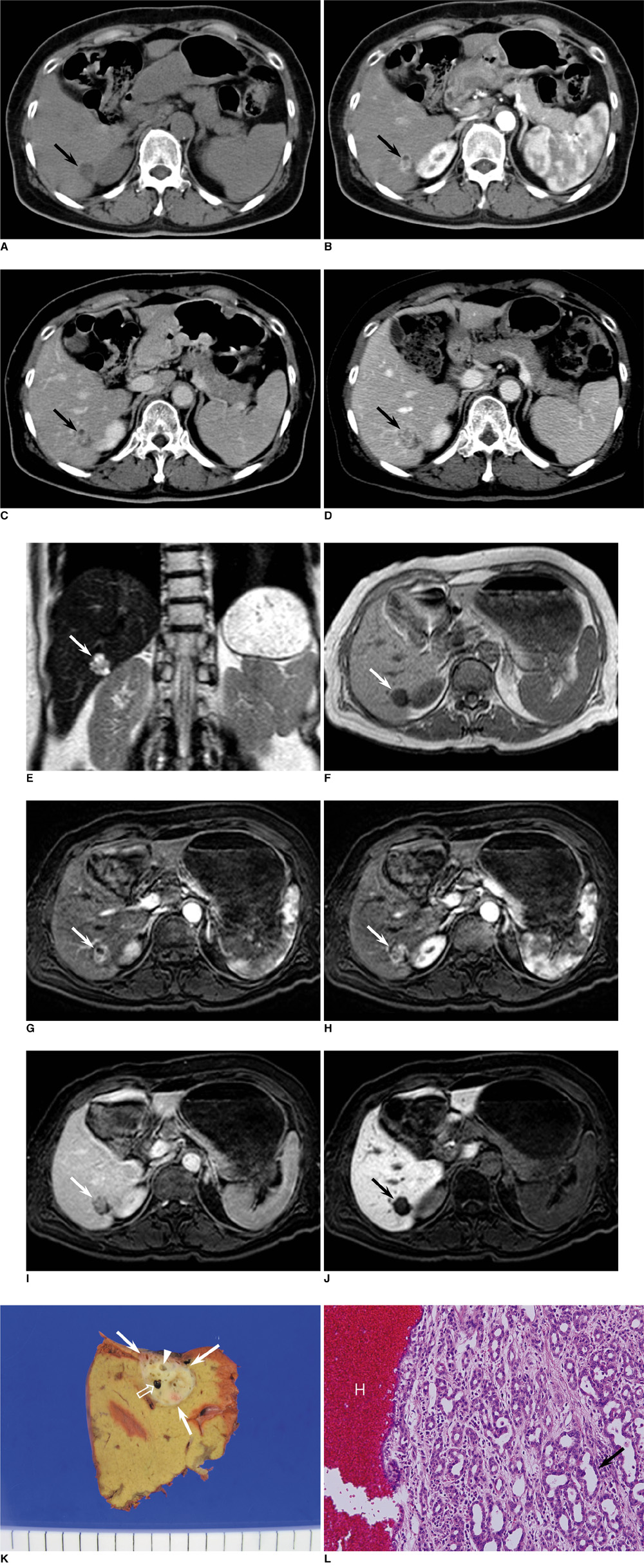
Fig. 1 Dynamic contrast-enhanced CT scans and follow-up MR images in 59-year-old woman with intrahepatic bile duct adenoma. A. Unenhanced CT scan shows well-defined low density mass measuring about 1.7 cm in periphery of posteroinferior segment of right hepatic lobe (arrow). B. Dynamic contrast-enhanced CT performed on mass shows heterogeneous enhancement (arrow) during hepatic arterial phase. Focal non-enhancing cystic portion is seen in anterior portion of mass. C. On equilibrium phase, mass shows relatively persistent enhancement (arrow). D. On equilibrium phase of follow-up CT scans obtained after seven months, tumor is slightly enlarged, measuring about 2.1 cm in diameter. E. Coronal T2-weighted half fourier acquisition single shot turbo spin echo (HASTE) image revealed that lesion has heterogeneous high signal intensity (arrow) with several small areas of bright signal intensity similar to that of fluid. F. On T1-weighted image, lesion shows homogeneous hypointensity (arrow). G. On dynamic contrast-enhanced T1-weighted images with fat saturation after administration of Gd-EOB-DTPA, upper portion of mass shows focal non-enhancing cystic portion with heterogeneous enhancement in remaining portion (arrow) during hepatic arterial phase. H. Lower portion of mass located 8 mm caudad to G shows heterogeneous enhancement during hepatic arterial phase. I. On equilibrium phase, mass shows relative hypointensity in comparison with normal liver parenchyma (arrow). J. On hepatobiliary phase obtained 20 minutes after contrast injection, mass shows distinct low signal intensity (arrow). K. Gross specimen shows well-circumscribed, non-encapsulated, yellowish white, subcapsular mass (white arrows). Multiple cystic changes (arrowhead) are seen in mass and focal hemorrhagic component (open arrow) is combined. L. Microscopically, mass consists of densely packed proliferation of simple tubular ducts (arrow) combined with hemorrhage (H). Cuboidal epithelium resembles that of interlobular bile ducts without cell atypia or mitotic activity (Hematoxylin & Eosin staining, ×200).
Reference
-
1. Allaire GS, Rabin L, Ishak KG, Sesterhenn IA. Bile duct adenoma. A study of 152 cases. Am J Surg Pathol. 1998. 12:708–715.2. Edmondson HA. Tumors of the liver and intrahepatic bile duct. Atlas of tumor pathology. 1958. Washington DC: Armed Forces Institute of Pathology;19–29. fascicle 25.3. Craig JR, Peters RL, Edmondson HA. Tumors of the liver and intrahepatic bile ducts. Atlas of tumor pathology. 1989. Washington DC: Armed Forces Institute of Pathology;56–62. 2nd series, fascicle 26.4. Tajima T, Honda H, Kuroiwa T, Yoshimitsu K, Irie H, Aibe H, et al. Radiologic features of intrahepatic bile duct adenoma: a look at the surface of the liver. J Comput Assist Tomogr. 1999. 23:690–695.5. Cho C, Rullis I, Rogers LS. Bile duct adenoma as liver nodules. Arch Surg. 1978. 113:272–274.6. Hornick JL, Lauwers GY, Odze RD. Immunohistochemistry can help distinguish metastatic pancreatic adenocarcinomas from bile duct adenomas and hamartomas of the liver. Am J Surg Pathol. 2005. 29:381–389.7. Levin SE, Dail DH, Saik RP. Bile duct adenomatosis of the liver: a misleading finding on surgical exploration of the abdomen. Am Surg. 1975. 41:106–108.8. Christine AL, Elizabeth M. Gastrointestinal and Liver Pathology. 2005. Philadelphia, PA: Churchill Livingstone;600–602.9. Bhathal PS, Hughers NR, Goodman AD. The so-called bile duct adenoma is a peribiliary gland hamartoma. Am J Surg Pathol. 1996. 20:858–864.10. Semelka RC, Hussain SM, Marcos HB, Woosley JT. Biliary hamartomas: solitary and multiple lesions shown on current MR techniques including gadolinium enhancement. J Magn Reson Imaging. 1999. 10:196–201.11. Govindarajan S, Peters RL. The bile duct adenoma. A lesion distinct from Meyenburg complex. Arch Pathol Lab Med. 1984. 108:922–924.12. Kobayashi T, Matsui O, Takashima T. Abdominal Radiology Study Group of Japan. A case of bile duct adenoma (Japanese). Atlas of diagnostic abdominal imaging. 1993. vol. 1. Osaka, Japan: Nihon Schering;26–27.13. Miyazaki Y, Honda H, Yamamichi K. A case of bile duct adenoma, its features of preoperative imaging (Japanese). 1997. In : 33rd annual meeting of Liver Cancer Study Group; –175.14. Maeda E, Uozumi K, Kato N, Akahane M, Inoh S, Inoue Y, et al. Magnetic resonance findings of bile duct adenoma with calcification. Radiat Med. 2006. 24:459–462.15. Honda H, Onitsuka H, Yasumori K, Hayashi T, Ochiai K, Gibo M, et al. Intrahepatic peripheral cholangiocarcinoma: two-phased dynamic incremental CT and pathologic correlation. J Comput Assist Tomogr. 1993. 17:397–402.16. Seale MK, Catalano OA, Saini S, Hahn PF, Sahani DV. Hepatobiliary-specific MR contrast agents: role in imaging the liver and biliary tree. Radiographics. 2009. 29:1725–1748.17. Skelly RT, Lee J, Sloan JM, Diamond T. Incidental bile duct adenomas in a patient with obstructive jaundice. Ulster Med J. 1999. 68:114–115.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Peribiliary Cysts with Intrahepatic Bile Duct Obstruction: A Case Report
- Histopathology of a benign bile duct lesion in the liver: Morphologic mimicker or precursor of intrahepatic cholangiocarcinoma
- Diffusion-Weighted MRI in Intrahepatic Bile Duct Adenoma Arising from the Cirrhotic Liver
- Intrahepatic Bile Duct Dilatation Caused by Pancreatic Pseudocyst: A Case Report
- RE: Diffusion-Weighted MRI in Intrahepatic Bile Duct Adenoma Arising from the Cirrhotic Liver
