The Results of B-scan Ultrasonography in Different Positions after Vitrectomy and Gas Tamponade
- Affiliations
-
- 1Department of Ophthalmology, Soonchunhyang University College of Medicine, Seoul, Korea. wismile@unitel.co.kr
- KMID: 1101912
- DOI: http://doi.org/10.3341/kjo.2007.21.2.100
Abstract
- PURPOSE: To determine the proper time frame in which to assess retinal attachment status and to evaluate the superior retinal attachment status by performing B-scan ultrasonography in different positions on patients who have undergone pars plana vitrectomy and gas tamoponade. METHODS: In this prospective study, 23 patients (23 eyes) who had undergone pars plana vitrectomy and gas tamponade were investigated between June 2005 and February 2006. SF6 (18%) was injected into the vitreous cavity of 15 eyes, and C3F8 (14%) was injected into the vitreous cavity of 8 eyes. At postoperative day 1, day 3, week 1, week 2, and week 4, B-scan ultrasonography was performed in the supine, sitting, prone, right decubitus, and left decubitus positions. RESULTS: The proper time to evaluate the retinal attachment status was three days post-operatively in 10 eyes (66.7%) with SF6 (18%) injections and two weeks post-operatively in six eyes (75%) that had C3F8 (14%) injections. The superior retinal attachment status can be evaluated from the summation of B-scan ultrasonography results performed in the right decubitus and left ducubitus positions. CONCLUSIONS: The proper time to evaluate the retinal attachment status was related to the degree of the gas absorption when performing B-scan ultrasonography after pars plana vitrectomy and gas tamponade. To evaluate the entire retina, it is useful to perform B-scan ultrasonograhy in the prone, right decubitus and left decubitus positions.
Keyword
MeSH Terms
Figure
-

Fig. 1 Photographs of B-scan ultrasonography with patients in different positions. (A) Supine position. (B) Sitting position. (C) Prone position. (D) Right decubitus position. (E) Left decubitus position.
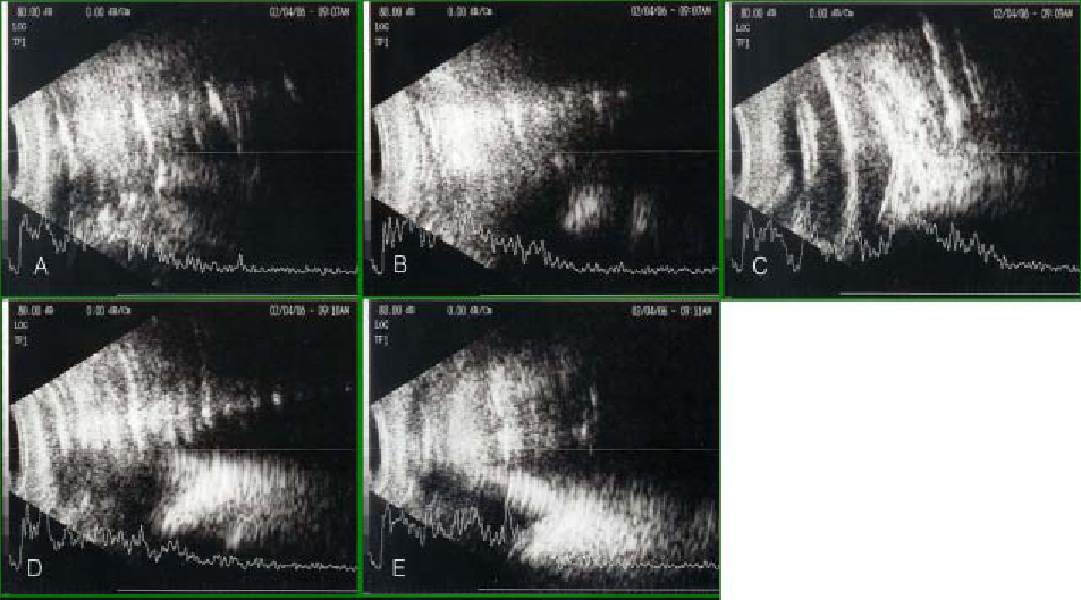
Fig. 2 On postoperative day 1, the results of B-scan ultrasonography while patients assumed different positions on eyes undergoing vitrectomy and an 18% SF6 gas tamponade. (A) Supine position: can not evaluate the retinal attachment status. (B) Sitting position: can not evaluate the retinal attachment status. (C) Prone position: can not evaluate the retinal attachment status. (D) Right decubitus position: can not evaluate the retinal attachment status. (E) Left decubitus position: can not evaluate the retinal attachment status.

Fig. 3 On postoperative day 3, the results of B-scan ultrasonography taken with patients in different positions on the eyes undergoing vitrectomy and an 18% SF6 gas tamponade. (A) Supine position: can not evaluate the retinal attachment status. (B) Sitting position: can evaluate the retinal attachment status greater than 180°. (C) Prone position: can not evaluate the retinal attachment status. (D) Right decubitus position: can evaluate the retinal attachment status greater than 180°. (E) Left decubitus position: can evaluate the retinal attachment status less than 180°.

Fig. 4 On postoperative day 7, results of B-scan ultrasonography with the patients in different positions of the eyes undergoing vitrectomy and an 18% SF6 gas tamponade. (A) Supine position: can not evaluate the retinal attachment status. (B) Sitting position: can evaluate the retinal attachment status greater than 180°. (C) Prone position: can not evaluate the retinal attachment status. (D) Right decubitus position: can evaluate the retinal attachment status greater than 180°. (E) Left decubitus position: can evaluate the retinal attachment status greater than 180°.

Fig. 5 At postoperative week 1, results of B-scan ultrasonography with patients in different positions on the eyes undergoing vitrectomy and using a 14% C3F8 gas tamponade. (A) Supine position: can not evaluate the retinal attachment status. (B) Sitting position: can not evaluate the retinal attachment status. (C) Prone position: can not evaluate the retinal attachment status. (D) Right decubitus position: can not evaluate the retinal attachment status. (E) Left decubitus position: can not evaluate the retinal attachment status.
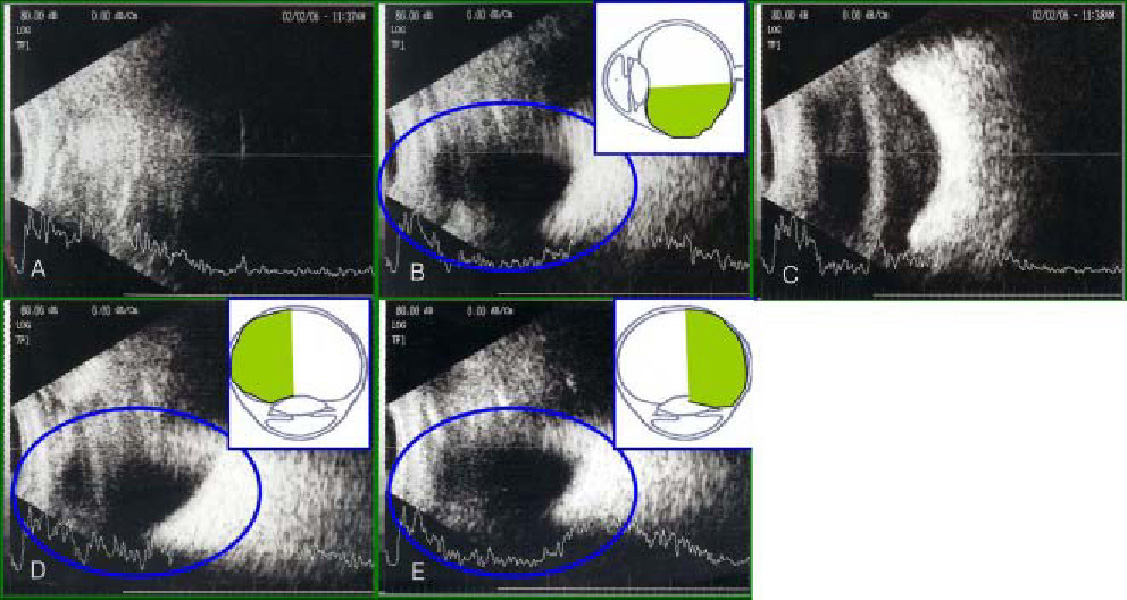
Fig. 6 At two weeks postoperatively, results of B-scan ultrasonography with patients assuming different positions on the eyes undergoing vitrectomy and using a 14% C3F8 gas tamponade. (A) Supine position: can not evaluate the retinal attachment status. (B) Sitting position: can evaluate the retinal attachment status greater than 180°. (C) Prone position: can not the retinal attachment status. (D) Right decubitus position: can evaluate the retinal attachment status greater than 180°. (E) Left decubitus position: can evaluate the retinal attachment status greater than 180°.

Fig. 7 Results of B-scan ultrasonography with the patient in the prone position on the eyes undergoing vitrectomy and using an 18% SF6 gas tamponade. (A) At postoperative day 1, (B) on postoperative day 2, (C) at postoperative day 3, (D) on postoperative day 4, (E) at postoperative day 5, (F) on postoperative day 6, (G) at postoperative day 10, (H) on postoperative day 11: the echogenic image that we thought was the retina proved to be the gas-fluid interface because this echogenic image has moved to the posterior pole from day to day.

Fig. 8 The false images on B-scan ultrasonography on the eyes filled with gas. (A) Posterior shadowing (red arrow). (B) Multiple reverberations (blue arrows).
Reference
-
1. Susanne S, Katharina K, Andreas W. Incidence of rhegmatogenous retinal detachment after vitrectomy in eyes of diabetic patients. Retina. 2006. 26:149–152.2. Han NS, Lee SB, Jo YJ. The results of primary vitrectomy for rhegmatogenous retinal detachment. J Korean Ophthalmol Soc. 2006. 47:55–61.3. Ahn JB, Huh K. Clinical analysis of vitrectomy for complication of proliferative diabetic retinopathy. J Korean Ophthalmol Soc. 1996. 37:1161–1167.4. Mochizuki Y, Yubota T, Hata Y, et al. Surgical results of combined pars plana vitrectomy, phacoemulsification, and intraocular lens implantation. Eur J Ophthalmol. 2006. 16:279–286.5. Treumer F, Bunse A, Rudolf M, Roider J. Pars plana vitrectomy, phacoemulsification and intraocular lens implantation. Comparison of clinical complications in a combined versus two-step surgical approach. Graefes Arch Clin Exp Ophthalmol. 2006. 244:808–815.6. Stephen JR, Ronald L, Green , Sandra FB. Diagnostic ophthalmic ultrasound. Retina. 2006. v. 1:4th ed. Baltimore: Elsevier Mosby;chap. 19.7. Wong Raymond F, Thomson John T. Prediction of the kinetics of disapperance of sulfur hexafluoride and perfluoropropane intraocular gas bubbles. Ophthalmology. 1988. 95:609–613.8. Thomson JT. Kinetics of intraocular gases. Arch Ophthalmol. 1989. 107:687–691.9. Lincoff H, Maise JM, Lincoff A. Intravitreal disappearance rates of four perfluorocarbon gases. Arch Ophthalmol. 1984. 102:928–929.10. Whitacre Macr M. B-scan ultrasonograghy of eyes containing intravitreal gas. Am J Ophthalmol. 1991. 112:272–277.11. Laing FC. Commonly encountered artifacts in clinical ultrasound. Seminars In Ultrasound. 1983. 4:27.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postural Effect on Intraocular Pressure in Gas-Filled Eyes after Vitrectomy
- Postoperative Refractive Error after Vitrectomy In Macular Hole Patients
- The Change in Corneal Endothelial Cell Density after Pars Plana Vitrectomy
- Postoperative Refractive Error by Using A-scan in Cataract Surgery After Vitrectomy
- The Effect of Gas Tamponade with Vitrectomy in Lamellar Macular Hole
