Long QT Syndrome and Torsade de Pointes Associated with Takotsubo Cardiomyopathy
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. matsalong@schmc.ac.kr
- KMID: 1094271
- DOI: http://doi.org/10.3346/jkms.2011.26.7.959
Abstract
- Prolongation of QTc interval associated with Takotsubo cardiomyopathy (TC) has previously been reported in published case series. We report an unusual case of a patient who presented with TC associated with long-QT syndrome and developed cardiac arrest secondary to torsade de pointes. Since QT prolongation and bradycardia persisted after the resolution of TC, the patient received permanent pacemaker. Since then additional event did not occur. QT prolongation and bradycardia could be persistent even after recovery of TC, and permanent pacemaker insertion may be a treatment option of long QT syndrome related with TC.
MeSH Terms
-
Aged
Bradycardia/diagnosis/therapy
Cardiac Pacing, Artificial
Coronary Angiography
Diagnosis, Differential
Electrocardiography
Female
Heart Arrest/diagnosis/etiology
Humans
Long QT Syndrome/*diagnosis/etiology
Takotsubo Cardiomyopathy/complications/*diagnosis/ultrasonography
Torsades de Pointes/*diagnosis/etiology
Figure
-
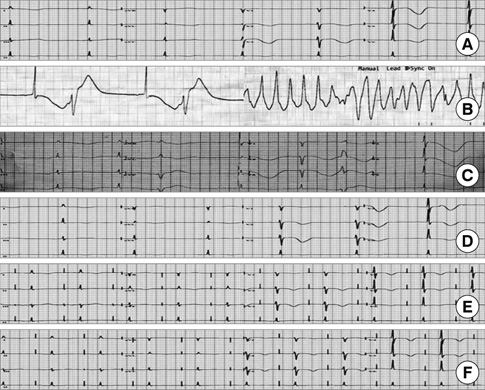
Fig. 1 Time course of ECG changes. (A) Admission electrocardiogram (ECG) shows T-wave inversion in precordial leads and a QTc interval of 580 ms. (B) ECG on the second day shows torsade de pointes initiated by a junctional rhythm with QT prolongation and R on T phenomenon. (C) ECG on the 4th day shows a junctional rhythm with QT prolongation (QTc = 653 ms) and R-on-T phenomenon (D) ECG on the 20th day shows a severe bradycardia with QT prolongation. (E, F) ECG and 3 months after pacemaker insertion still shows QT prolongation and T-wave inversion in precordial leads.

Fig. 2 Two-dimensional echocardiogrphic findings on admission and 2 weeks later. On admission the left ventricular mid wall and apex showed ballooning akinesis. (A) End-diastole. (B) End-systole. Two weeks later, these findings disappeared, and left ventricular contraction nearly normalized. (C) End-diastole, (D) End-systole.

Fig. 3 (A, B) Coronary angiogram shows only a small atheroma.
Reference
-
1. Eckhardt L, Brugada P, Morgan J, Breithardt G. Camm AJ, Luscher TF, Serruys PW, editors. Ventricular tachycardia. The ESC textbook of cardiovascular medline. 2006. Oxford: Blackwell;949–972.2. Yoshida T, Hibino T, Kako N, Murai S, Oguri M, Kato K, Yajima K, Ohte N, Kimura G. A pathophysiologic study of tako-tsubo cardiomyopathy with F-18 fluorodeoxyglucose positron emission tomography. Eur Heart J. 2007. 28:2598–2604.3. Matsuoka K, Okubo S, Fujii E, Uchida F, Kasai A, Aoki T, Makino K, Omichi C, Fujimoto N, Ohta S, Sawai T, Nakano T. Evaluation of the arrhythmogenecity of stress induced 'Takotsubo cardiomyopathy' from the time course of the 12-lead surface electrocardiogram. Am J Cardiol. 2003. 92:230–233.4. Samuelov-Kinori L, Kinori M, Kogan Y, Swartzon M, Shalev H, Guy D, Fereninou F, Mashav N, Sadeh B, Atzmony L, Kliuk-Ben-Basat O, Steinvil A, Justo D. Takotsubo cardiomyopathy and QT interval prolongation: who are the patients at risk for torsades de pointes? J Electrocardiol. 2009. 42:353–357.5. Denney SD, Lakkireddy DR, Khan IA. Long QT syndrome and torsade de pointes in transient left ventricular apical ballooning syndrome. Int J Cardiol. 2005. 100:499–501.6. Inoue M, Kanaya H, Matsubara T, Uno Y, Yasuda T, Miwa K. Complete atrioventricular block associated with takotsubo cardiomyopathy. Circ J. 2009. 73:589–592.7. Mahida S, Dalageorgou C, Behr ER. Long-QT syndrome and torsades de pointes in a patient with Takotsubo cardiomyopathy: an unusual case. Europace. 2009. 11:376–378.8. Sasaki O, Nishioka T, Akima T, Tahata H, Okamoto Y, Akanuma M, Uehata A, Takase B, Katsushika S, Isojima K, Ohtomi S, Yoshimot N. Association of takotsubo cardiomyopathy and long QT syndrome. Circ J. 2006. 70:1220–1222.9. Kurisu S, Inoue I, Kawagoe T, Ishihara M, Shimatani Y, Nakama Y, Ohkawa K, Maruhashi T, Kagawa E, Dai K, Aokage T. Torsade de pointes associated with bradycardia and takotsubo cardiomyopathy. Can J Cardiol. 2008. 24:640–642.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Stress Cardiomyopathy Complicated by Torsades de Pointes in a Patient with Acute Colitis: A Case Report
- Postanesthetic torsade de pointes in a patient with unrecognized long QT syndrome: A case report
- A Case of Torsade de Pointes after Combined Use of Terfenadine and Itraconazole
- A Case of Torsade de Pointes Associated with Hypopituitarism due to Hemorrhagic Fever with Renal Syndrome
- QT Prolongation and Life Threatening Ventricular Tachycardia in a Patient Injected With Intravenous Meperidine (Demerol(R))
