Concordant or Discordant? Imaging-Pathology Correlation in a Sonography-Guided Core Needle Biopsy of a Breast Lesion
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 120-752, Korea. ekkim@yuhs.ac
- 2Department of Radiology, Bundang CHA Hospital, CHA University, Gyeonggi-do 463-712, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Seoul 120-752, Korea.
- 4Department of Pathology, Bundang CHA Hospital, CHA University, Gyeonggi-do 463-712, Korea.
- KMID: 1088569
- DOI: http://doi.org/10.3348/kjr.2011.12.2.232
Abstract
- An imaging-guided core needle biopsy has been proven to be reliable and accurate for the diagnosis of both benign and malignant diseases of the breast, and has replaced surgical biopsy. However, the possibility of a false-negative biopsy still remains. Imaging-pathology correlation is of critical importance in imaging-guided breast biopsies to detect such a possible sampling error and avoid a delay in diagnosis. We will review five possible categories and corresponding management after performing an imaging-pathology correlation in a sonography-guided core needle biopsy of a breast lesion, as well as illustrate the selected images for each category in conjunction with the pathologic finding. Radiologists should be familiar with the imaging features of various breast pathologies and be able to appropriately correlate imaging findings with pathologic results after a core needle biopsy.
Keyword
MeSH Terms
Figure
-
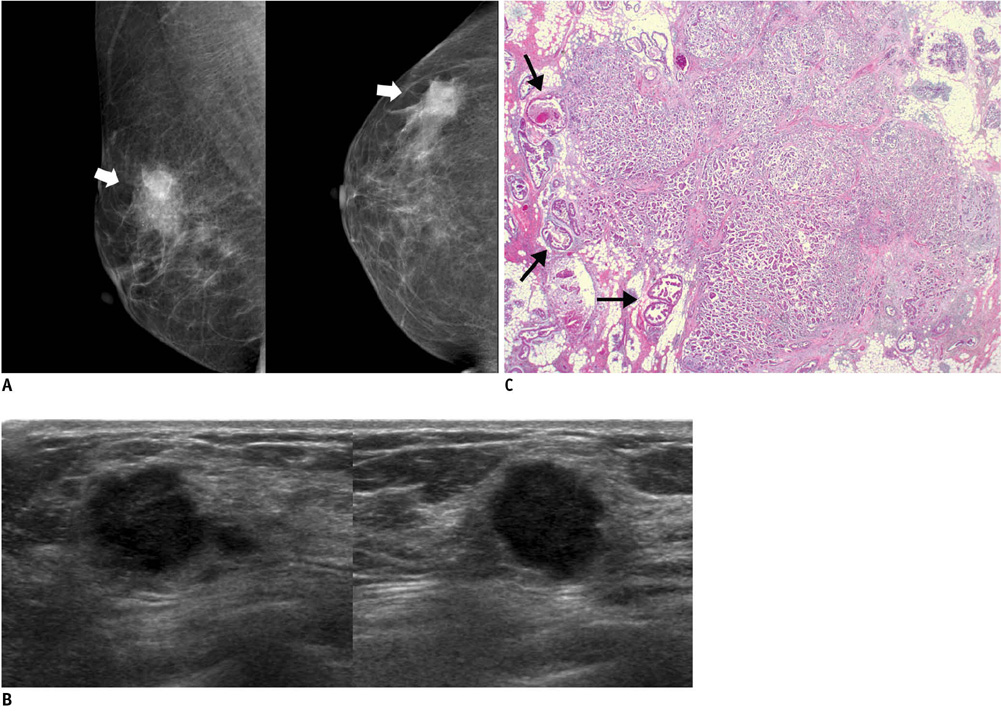
Fig. 1 46-year-old woman with palpable mass in her right breast. A. On mammography (left: mediolateral oblique view, right: craniocaudal view), irregular ill-defined hyperdense mass (arrows) is seen on area corresponding to palpable abnormality. B. On sonography (left: transverse view, right: longitudinal view), mass is determined to be round microlobulated hypoechoic mass with nonparallel orientation and classified as BI-RADS category 4c. Result of sonography-guided 14-gauge core needle biopsy are consistent with invasive ductal carcinoma, which is considered as concordant malignancy. C. Histologic features on low power view indicate invasive ductal carcinoma with peripheral intraductal component (arrows) without microcalcification. Surrounding breast parenchyma shows fatty changes (Hematoxylin & Eosin staining; original magnification, × 10).
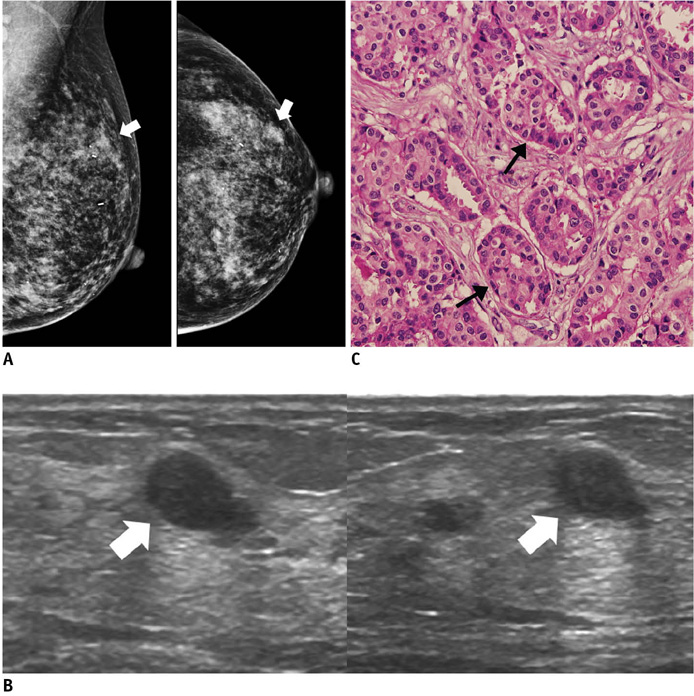
Fig. 2 46-year-old woman with mass in her left breast. A. On mammography (left: mediolateral oblique view, right: craniocaudal view), there is focal asymmetry (arrows) in upper outer portion of left breast. B. On sonography (left: transverse view, right: longitudinal view), oval circumscribed hypoechoic mass (arrows) is seen and classified as BI-RADS category 3. Sonography-guided 14-gauge core needle biopsy was performed at request of patient and pathologic result is consistent with invasive ductal carcinoma, which is considered as discordant malignancy. C. Photomicrograph of microscopic specimen after surgical excision shows relatively well-differentiated tumor cell nests dispersed in desmoplastic stroma (arrows). No intraductal component was seen in submitted specimen. Final diagnosis was invasive ductal carcinoma (Hematoxylin & Eosin staining; original magnification, × 100).
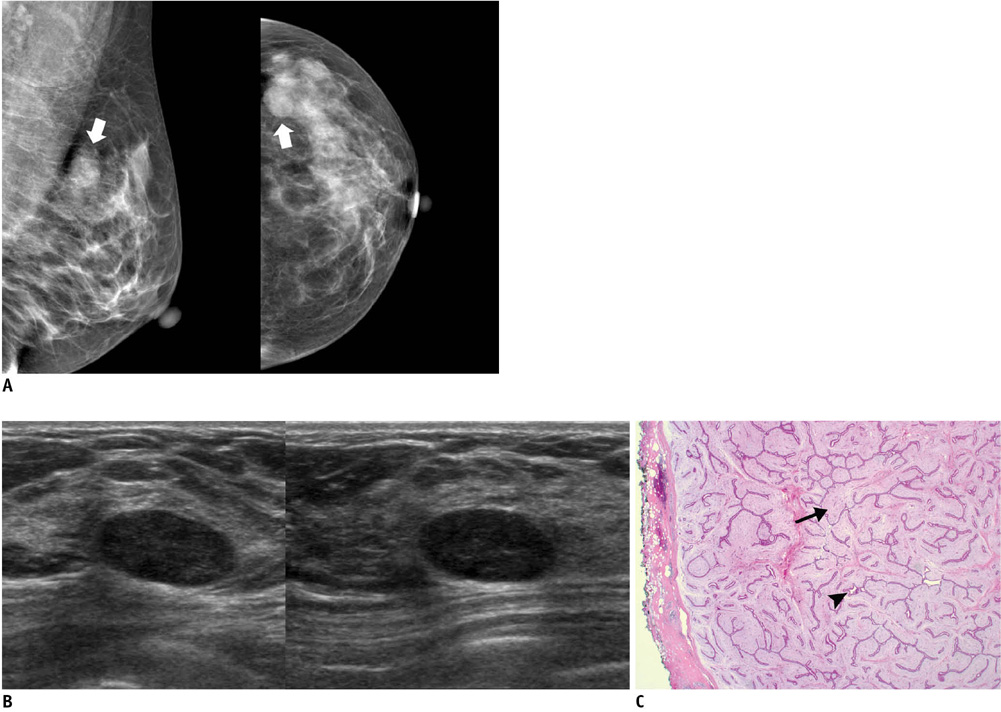
Fig. 3 45-year-old woman with mass in her left breast. A. On mammography (left: mediolateral oblique view, right: craniocaudal view), oval circumscribed mass (arrows) is seen in upper outer portion of her left breast. B. On sonography (left: transverse view, right: longitudinal view), oval circumscribed hypoechoic mass is seen and classified as BI-RADS category 3. Sonography-guided 14-gauge core needle biopsy was performed at request of patient and pathologic result indicated fibroadenoma, which is considered to be concordant benign lesion. However, in lieu of follow-up image, surgical excision was performed. C. Photomicrograph of microscopic specimen after surgical excision shows sharply defined border with both glandular (arrowhead) and stromal proliferation (arrow), mainly showing intracanalicular growth pattern. Final diagnosis was fibroadenoma (Hematoxylin & Eosin staining; original magnification, × 10).
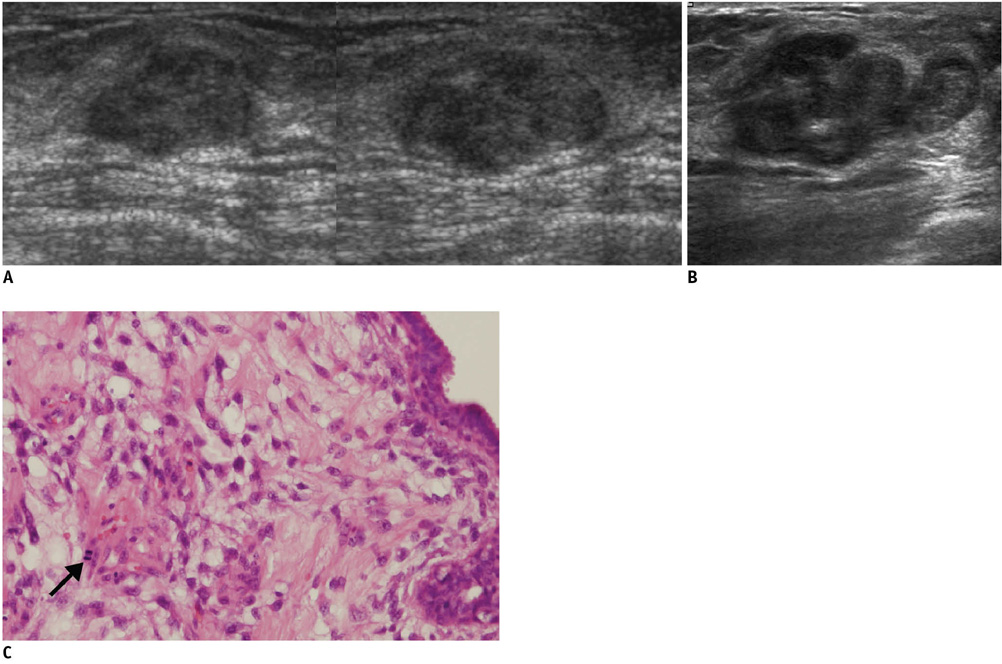
Fig. 4 56-year-old woman with palpable mass in her left breast. A. On sonography (left: transverse view, right: longitudinal view), oval circumscribed hypoechoic mass is seen classified as BI-RADS category 3. Sonography-guided 14-gauge core needle biopsy was performed at request of physician and pathologic result was fibroadenoma, which was considered as concordant benign. B. At 6-month follow-up, mass was found to have grown along with development of calcifications and cystic change. C. Final pathological diagnosis of surgically excised lesion was malignant phyllodes tumor. Hypercellular stromal cells with atypia and mitosis (arrow) are noted (Hematoxylin & Eosin staining; original magnification, × 100).
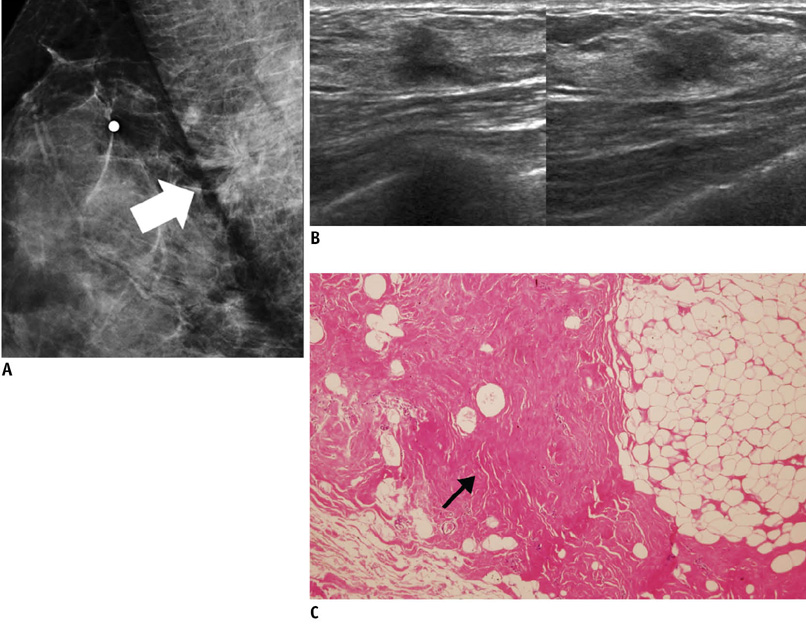
Fig. 5 52-year-old woman with palpable mass in her right breast. A. On mediolateral oblique view of mammography, there is architectural distortion (arrow) in right breast. B. On sonography (left: transverse view, right: longitudinal view), irregular spiculated hypoechoic mass is seen and classified as BI-RADS category 4c. Result of sonography-guided 14-gauge core needle biopsy indicates stromal fibrosis, which was considered as discordant benign. C. Surgically excised specimen reveals widespread dense stromal fibrosis without ductal cell hyperplasia (arrow). Final diagnosis was stromal fibrosis (Hematoxylin & Eosin staining; original magnification, × 100).
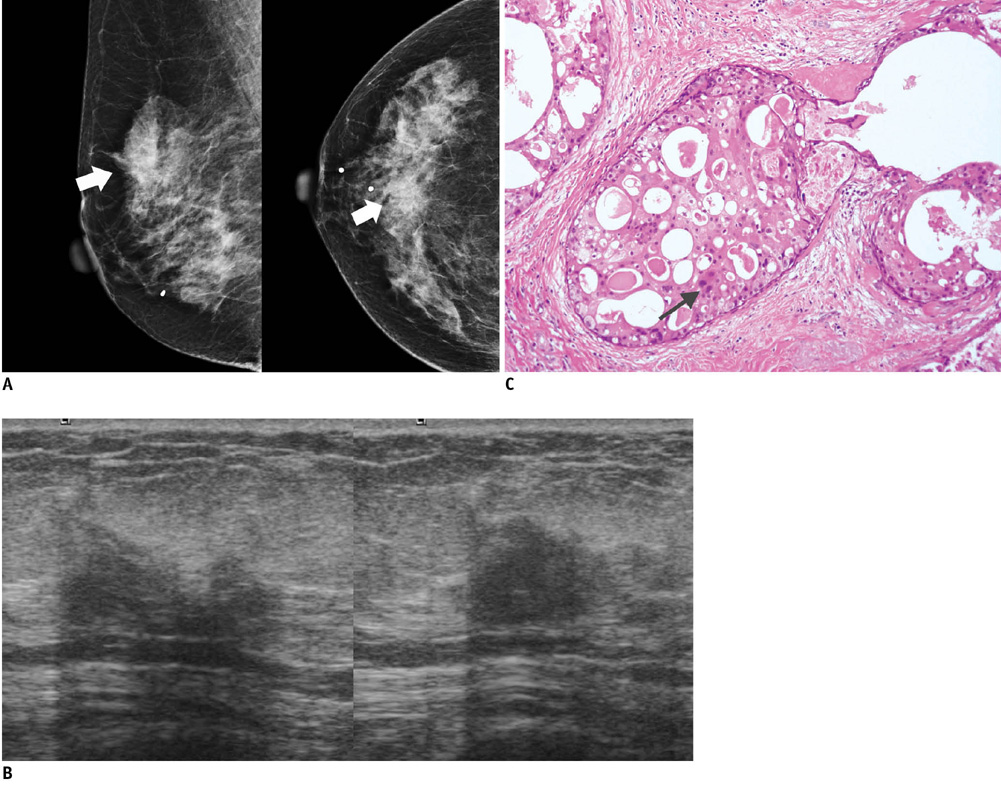
Fig. 6 65-year-old woman with mass in her right breast. A. On mammography (left: mediolateral oblique view, right: craniocaudal view), indistinct mass (arrows) is present in right breast. B. On sonography (left: transverse view, right: longitudinal view), oval hypoechoic mass with angular or ill-defined margin is seen and classified as BI-RADS category 4c. After performing sonography-guided 14-gauge core needle biopsy, biopsy result was fibrocystic change, which is considered as discordant benign. C. Surgical specimen shows lesion consisting of extensive ductal carcinoma in situ with lobular cancerization. Relatively monotonous cells with low-grade nuclei and abundant, eosinophilic cytoplasm in form of cribriform pattern (arrow) are noted (Hematoxylin & Eosin staining; original magnification, × 200).

Fig. 7 36-year-old woman with palpable mass in her right breast. A. On sonography (left: transverse view, right: longitudinal view), round microlobulated hypoechoic mass with microcalcifications and nonparallel orientation (arrowheads) is seen and classified as BI-RADS category 4c. Results of sonography-guided 14-gauge core needle biopsy indicate presence of stromal sclerosis, which is considered as discordant benign. B. Final diagnosis after surgical excision was invasive ductal carcinoma. Photomicrograph of microscopic specimen after surgical excision shows carcinoma within sclerotic stroma (Hematoxylin & Eosin staining; original magnification, × 40).

Fig. 8 40-year-old woman with palpable mass in her left breast. A. On sonography (left: transverse view, right: longitudinal view), oval microlobulated hypoechoic mass with echogenic halo and nonparallel orientation is seen and classified as BI-RADS category 4b. Result of sonography-guided 14-gauge core needle biopsy indicates fibroadenoma, which is considered as discordant benign. B. Surgically excised specimen reveals well circumscribed, lobulated mass with tumoral florid adenosis, consistent with adenosis tumor (Hematoxylin & Eosin staining; original magnification, × 100).
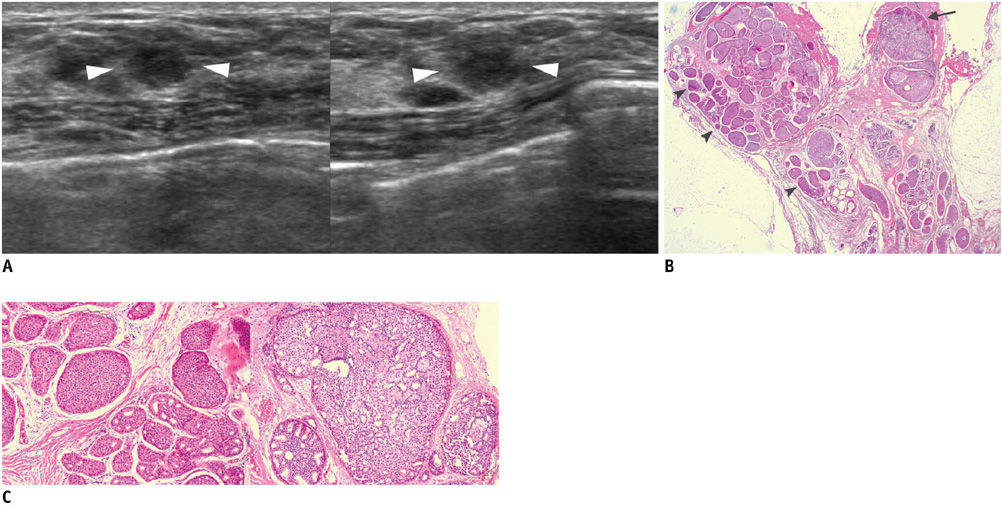
Fig. 9 49-year-old woman with mass in her left breast. A. On sonography (left: transverse view, right: longitudinal view), oval ill-defined hypoechoic mass (arrowheads) is seen and classified as BI-RADS category 4a. Results of sonography-guided 14-gauge core needle biopsy indicate presence of atypical intraductal papilloma and atypical ductal hyperplasia, which is considered as borderline or high-risk. B, C. At photomicrograph of microscopic specimen after surgical excision (B: Hematoxylin & Eosin staining; original magnification, × 10), ductal carcinoma in situ (upper and lower left; arrowheads) and atypical intraductal papilloma (upper right; arrow) are shown. At high-power field (C: Hematoxylin & Eosin staining; original magnification, × 100), ductal carcinoma in situ with low grade, cribriform pattern (left), as well as an atypical papilloma with central intraductal papilloma pattern and peripheral atypical ductal hyperplasia pattern in largest duct (right) are shown.
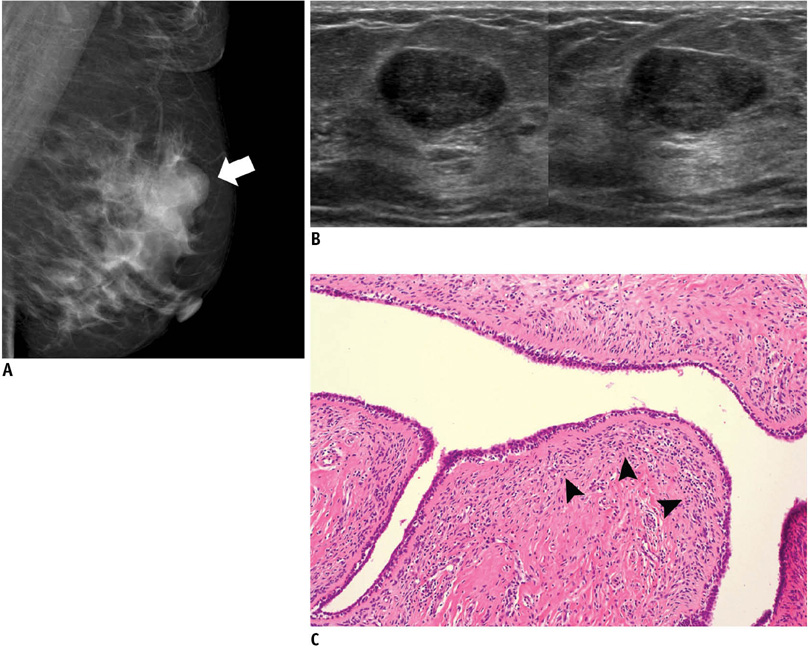
Fig. 10 49-year-old woman with palpable mass in her left breast. A. On mediolateral oblique view of mammography, oval obscured mass (arrow) is shown in left breast. B. On sonography (left: transverse view, right: longitudinal view), oval circumscribed hypoechoic mass is seen and classified as BI-RADS category 3. Results of sonography-guided 14-gauge core needle biopsy performed by request of physician indicate presence of benign phyllodes tumor, which is considered as borderline or high-risk. C. Photomicrograph of microscopic specimen after surgical excision shows relatively ill-defined border, elongated epithelial-lined clefts, and mild increase in stromal cellularity with periductal stromal accentuation (arrowheads), consistent with benign phyllodes tumor (Hematoxylin & Eosin staining; original magnification, × 100).
Reference
-
1. Bassett LW, Mahoney MC, Apple SK. Interventional breast imaging: current procedures and assessing for concordance with pathology. Radiol Clin North Am. 2007. 45:881–894.2. Youk JH, Kim EK, Kim MJ, Lee JY, Oh KK. Missed breast cancers at US-guided core needle biopsy: how to reduce them. Radiographics. 2007. 27:79–94.3. Liberman L, Drotman M, Morris EA, LaTrenta LR, Abramson AF, Zakowski MF, et al. Imaging-histologic discordance at percutaneous breast biopsy. Cancer. 2000. 89:2538–2546.4. Parikh J, Tickman R. Image-guided tissue sampling: where radiology meets pathology. Breast J. 2005. 11:403–409.5. Liberman L. Percutaneous image-guided core breast biopsy. Radiol Clin North Am. 2002. 40:483–500.6. Comstock CE. Feig SA, editor. US-guided interventional procedures. 2005 Syllabus: categorical course in diagnostic radiology-breast imaging. 2005. Oak Brook, IL: Radiological Society of North America;155–168.7. Whitman GJ, Erguvan-Dogan B, Yang WT, Wilson J, Patel P, Krishnamurthy S. Ultrasound-guided breast biopsies. Ultrasound Clin. 2006. 1:603–615.8. Starvros AT. McAllister L, Donnellan K, Martin SP, Rothschild R, editors. False-negative and false-positive examinations. Breast ultrasound. 2004. Philadelphia, PA: Lippincott Williams & Wilkins;947–978.9. Kim MJ, Kim EK, Lee JY, Youk JH, Park BW, Kim SI, et al. Breast lesions with imaging-histologic discordance during US-guided 14G automated core biopsy: can the directional vacuum-assisted removal replace the surgical excision? Initial findings. Eur Radiol. 2007. 17:2376–2383.10. Kim EK, Ko KH, Oh KK, Kwak JY, You JK, Kim MJ, et al. Clinical application of the BI-RADS final assessment to breast sonography in conjunction with mammography. AJR Am J Roentgenol. 2008. 190:1209–1215.11. Lazarus E, Mainiero MB, Schepps B, Koelliker SL, Livingston LS. BI-RADS lexicon for US and mammography: interobserver variability and positive predictive value. Radiology. 2006. 239:385–391.12. Raza S, Chikarmane SA, Neilsen SS, Zorn LM, Birdwell RL. BI-RADS 3, 4, and 5 lesions: value of US in management--follow-up and outcome. Radiology. 2008. 248:773–781.13. Lee HJ, Kim EK, Kim MJ, Youk JH, Lee JY, Kang DR, et al. Observer variability of Breast Imaging Reporting and Data System (BI-RADS) for breast ultrasound. Eur J Radiol. 2008. 65:293–298.14. American College of Radiology. American College of Radiology. Breast imaging reporting and data system-mammography. Breast imaging reporting and data system. 2003. 4th ed. Reston, VA: American College of Radiology.15. Bent CK, Bassett LW, D'Orsi CJ, Sayre JW. The positive predictive value of BI-RADS microcalcification descriptors and final assessment categories. AJR Am J Roentgenol. 2010. 194:1378–1383.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breast Lesions with Discordant Results on Ultrasound-guided Core Needle Biopsy
- Sonographically-Guided 14-Gauge Core Needle Biopsy for Papillary Lesions of the Breast
- Clinicopathologic Features of the Papillary Breast Lesions Diagnosed on Ultrasonography-guided Core Needle Biopsy
- The Clinical Experience of an Ultrasound-guided Vacuum-assisted Resection (Mammotome) for Benign Breast Lesions through a Core Needle Biopsy
- Pseudoaneurysm of the Breast after Core Needle Biopsy: A Case Report
