Early Hepatocellular Carcinoma: Three-Phase Helical CT Features of 16 Patients
- Affiliations
-
- 1Department of Radiology and Center of Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. wjlee@skku.edu
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Radiology, Korea University Guro Hospital, Seoul, Korea.
- 4Department of Radiology, Bucheon Hospital, Soonchunhyang University School of Medicine, Gyeonggi-do, Korea.
- KMID: 1076458
- DOI: http://doi.org/10.3348/kjr.2008.9.4.325
Abstract
OBJECTIVE
To evaluate the three-phase helical CT features of early hepatocellular carcinomas, based on the new Japanese classification. MATERIALS AND METHODS: Over the course of an eight-year period, we collected 16 pathologically proven early hepatocellular carcinomas from 16 patients having undergone a three-phase helical CT prior to surgery. The three-phase CT images were acquired at 20-35 sec (arterial phase), 70 sec (portal phase), and 180 sec (equilibrium phase) from the begining of intravenous injection of contrast material. All the CT images were retrospectively analyzed by two radiologists in consensus, based on their description of morphologic (size, margin, fibrous capsule and mosaic pattern) and enhancement patterns of tumors. RESULTS: Only seven (44%) of the 16 early hepatocellular carcinomas having undergone a CT were described (mean diameter, 1.2 cm; range, 0.4-2.5 cm). All the tumors had an ill-defined margin with no fibrous capsule. The mosaic pattern was found in only one tumor. Only three (43%) of the seven tumors detected on CT were hyperattenuating during the arterial phase. The four remaining tumors (25%) were hypoattenuating throughout the three phases. CONCLUSION: Despite the higher resolution provided by the three phase scans, the contrast-enhanced CT provides only limited detection of the variable morphologic and enhancement features of early hepatocellular carcinomas.
MeSH Terms
Figure
-
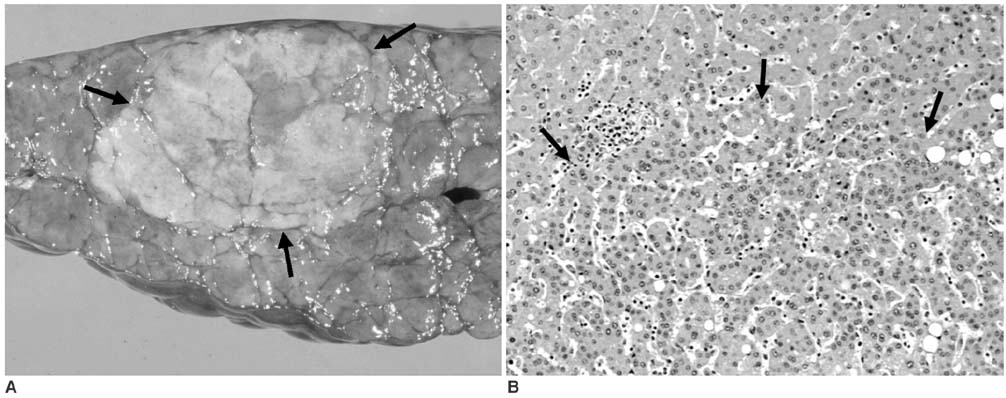
Fig. 1 62-year-old man with early hepatocellular carcinoma located in right hepatic lobe. A. Photograph of resected gross specimen shows 2.2-cm, slightly yellowish nodule (arrows) with indistinct margin. B. Photomicrograph of same specimen shows tumor cells of well-differentiated hepatocellular carcinoma in lower half of field (below arrows). Note that tumor cells appear to replace normal hepatocytes without clear demarcation (i.e. replacement growth - Hematoxylin & Eosin staining, ×100).

Fig. 2 48-year-old man with early hepatocellular carcinoma of so called "nodule in nodule lesion" (i.e. early advanced hepatocellular carcinoma) located in right hepatic lobe. A. Axial helical CT scan of liver during arterial phase shows 1.8-cm, hypoattenuating nodule with indistinct margin (arrows) located in segment VI of right hepatic lobe. Note faintly enhancing portion (arrowheads) within hypoattenuating nodule, representing mosaic pattern (nodule-in-nodule pattern). B, C. Corresponding portal (B) and equilibrium (C) phase CT scans show same hypoattenuating nodule (arrows). Faintly enhancing portion observed in arterial phase image becomes isoattenuating during later phases. D. Photograph of Hematoxylin and Eosin stained resected specimen shows same nodule (arrows) with indistinct margin and uneven fatty change. Note small nodule (arrowheads) in its upper part (i.e. mosaic pattern - nodule-in-nodule pattern), which corresponds to faintly enhancing portion observed in arterial phase CT image. Histopathologic findings revealed that whole nodule was composed of tumor cells of well-differentiated hepatocellular carcinoma, while small nodule was composed of moderately differentiated hepatocellular carcinoma.

Fig. 3 54-year-old man with early hepatocellular carcinoma located in right hepatic lobe. A. Three-phase helical CT image obtained during arterial phase shows 0.8cm, faintly hyperattenuating nodule with indistinct margin (arrows) in segment VI of right hepatic lobe. B, C. Corresponding portal (B) and equilibrium (C) phase CT scans show that hyperattenuating nodule observed in arterial phase becomes isoattenuating during portal and equilibrium phases (arrows).
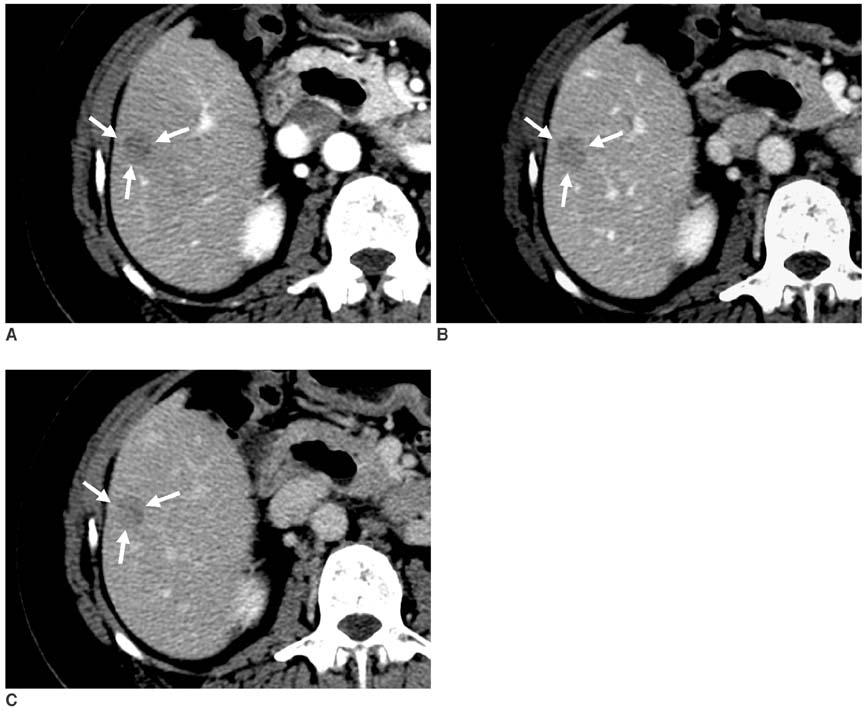
Fig. 4 51-year-old woman with early hepatocellular carcinoma located in right hepatic lobe. A. Three-phase helical CT image obtained during arterial phase shows 1.3-cm, hypoattenuating nodule with indistinct margin (arrows) in segment V of right hepatic lobe. B, C. Corresponding portal (B) and equilibrium (C) phase CT scans show same hypoattenuating nodule (arrows) in segment V of right hepatic lobe.
Reference
-
1. Sakamoto M, Hirohashi S, Shimosato Y. Early stages of multistep hepatocarcinogenesis: adenomatous hyperplasia and early hepatocellular carcinoma. Hum Pathol. 1991. 22:172–178.2. Kanai T, Hirohashi S, Upton MP, Noguchi M, Kishi K, Makuuchi M, et al. Pathology of small hepatocellular carcinoma. A proposal for new gross classification. Cancer. 1987. 60:810–819.3. Inoue K, Takayama T, Higaki T, Watanabe Y, Makuuchi M. Clinical significance of early hepatocellular carcinoma. Liver Transpl. 2004. 10:S16–S19.4. Yamamoto M, Takasaki K, Otsubo T, Katsuragawa H, Kataqiri S, Yoshitoshi K, et al. Favorable surgical outcomes in patients with early hepatocellular carcinoma. Ann Surg. 2004. 239:395–399.5. Takayama T, Makuuchi M, Hirohashi S, Sakamoto M, Yamamoto J, Shimada K, et al. Early hepatocellular carcinoma as an entity with a high rate of surgical cure. Hepatology. 1998. 28:1241–1246.6. The Liver Cancer Study Group of Japan. The general rules for the clinical and pathological study of primary liver cancer. 2000. 4th ed. Tokyo: Kanehara;13. [in Japanese].7. The Liver Cancer Study Group of Japan. The general rules for the clinical and pathological study of primary liver cancer. 2003. 2th ed. Tokyo: Kanehara;15.8. Takayasu K, Furukawa H, Wakao F, Muramatsu Y, Abe H, Terauchi T, et al. CT diagnosis of early hepatocellular carcinoma: sensitivity, findings, and CT-pathologic correlation. AJR Am J Roentgenol. 1995. 164:885–890.9. Takayasu K, Muramatsu Y, Furukawa H, Wakao F, Moriyama N, Takayama T, et al. Early hepatocellular carcinoma: appearance at CT during arterial portography and CT arteriography with pathologic correlation. Radiology. 1995. 194:101–105.10. Takayasu K, Muramatsu Y, Mizuguchi Y, Moriyama N, Ojima H. Imaging of early hepatocellular carcinoma and adenomatous hyperplasia (dysplastic nodules) with dynamic CT and a combination of CT and angiography: experience with resected liver specimens. Intervirology. 2004. 47:199–208.11. Yoshikawa J, Matsui O, Takashima T, Ida M, Takanaka T, Kawamura I, et al. Fatty metamorphosis in hepatocellular carcinoma: radiologic features in 10 cases. AJR Am J Roentgenol. 1988. 151:717–720.12. Stevens WR, Gulino SP, Batts KP, Stephens DH, Johnson CD. Mosaic pattern of hepatocellular carcinoma: histologic basis for a characteristic CT appearance. J Comput Assist Tomogr. 1996. 20:337–342.13. Rim KS, Sakamoto M, Watanabe H, Matsuno Y, Nakanishi Y, Mukai K, et al. Pathology and DNA cytophotometry of small hepatocellular carcinoma with a nodule-in-nodule appearance --evidence for stepwise progression of hepatocellular carcinoma. Jpn J Clin Oncol. 1993. 23:26–33.14. Winter TC 3rd, Takayasu K, Muramatsu Y, Furukawa H, Wakao F, Koga H, et al. Early advanced hepatocellular carcinoma: evaluation of CT and MR appearance with pathologic correlation. Radiology. 1994. 192:379–387.15. International Working Party. Terminology of nodular hepatocellular lesions. Hepatology. 1995. 22:983–993.16. Ueda K, Terada T, Nakanuma Y, Matsui O. Vascular supply in adenomatous hyperplasia of the liver and hepatocellular carcinoma: a morphometric study. Hum Pathol. 1992. 23:619–626.17. Kojiro M. Focus on dysplastic nodules and early hepatocellular carcinoma: an Eastern point of view. Liver Transpl. 2004. 10:S3–S8.18. Kutami R, Nakashima Y, Nakashima O, Shiota K, Kojiro M. Pathomorphologic study on the mechanism of fatty change in small hepatocellular carcinoma of humans. J Hepatol. 2000. 33:282–289.19. Kojiro M, Sugihara S, Nakashima O. Okuda K, Tobe T, Kitagawa T, editors. Pathomorphologic characteristics of early hepatocellular carcinoma. Early detection and treatment of liver cancer(Gann monograph on cancer research, vol.38.). 1991. Tokyo: Japan Scientific Societies Press;29–37.20. Stevens WR, Johnson CD, Stephens DH, Batts KP. CT findings in hepatocellular carcinoma: correlation of tumor characteristics with causative factors, tumor size, and histologic tumor grade. Radiology. 1994. 191:531–537.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection of Hepatocelluar Carcinoma on Triple-Phase Images of Liver Using Multi-Detector Row Helical CT
- Difference in Early Postoperative Recurrence Rate of Hepatocellular Carcinoma According to the Imaging Modalities Used for Preoperative Staging : Comparison Between CTAP and CTHA, Lipiodol CT and Three Phase Helical CT
- CT Detection of Hepatocellular Carcinoma in Advanced Liver Cirrhosis: Correlation of Helical CT and Explanted Liver
- Spiral CT of Hepatocellular Carcinoma: Correlation of CT Scans during the Arterial Phase with Angiography
- Enhancement Pattern of Hepatocellular Carcinoma on Triphasic Helical CT: Quantitative Study
