Fetal Topographical Anatomy of the Pancreatic Head and Duodenum with Special Reference to Courses of the Pancreaticoduodenal Arteries
- Affiliations
-
- 1Departement of Surgery, Chonbuk National University Medical School, Jeonju, Korea. hcyu@chonbuk.ac.kr
- 2Departement of Anatomy, Chonbuk National University Medical School, Jeonju, Korea.
- 3Departement of Gastroenterologic Surgery, Yamagata University School of Medicine, Yamagata, Japan.
- 4Departement of Anatomy, Sapporo Medical University School of Medicine, Sapporo, Japan.
- 5Division of Internal Medicine, Iwamizawa Koujin-kai Hospital, Iwamizawa, Japan.
- KMID: 1074992
- DOI: http://doi.org/10.3349/ymj.2010.51.3.398
Abstract
- PURPOSE
The purpose of this study is to provide better understanding as to how the "double" vascular arcades, in contrast to other intestinal marginal vessels, develop along the right margin of the pancreatic head.
MATERIALS AND METHODS
In human fetuses between 8-30 weeks, we described the topographical anatomy of the vessels, bile duct, duodenum as well as the ventral and dorsal primordia of the pancreatic head with an aid of pancreatic polypeptide immunohisto-chemistry.
RESULTS
The contents of the hepatoduodenal ligament crossed the superior side of the pylorus. Moreover, the right hepatic artery originating from the superior mesenteric artery ran along the superior aspect of the pancreatic head. An arterial arcade, corresponding to the posterior pancreaticoduodenal arteries, encircled the superior part of the pancreatic head, whereas another arcade, corresponding to the anterior pancreaticoduodenal arteries, surrounded the inferior part. The dorsal promordium of the pancreas surrounded and/or mixed the ventral primordium at 13-16 weeks. Thus, both arterial arcades were likely to attach to the dorsal primordium.
CONCLUSION
The fetal anatomy of the pancreaticoduodenal vascular arcades as well as that of the hepatoduodenal ligament were quite different from adults in topographical relations. Thus, in the stage later than 30 weeks, further rotation of the duodenum along a horizontal axis seemed to be required to move the pylorus posterosuperiorly and to reflect the superior surface of the pancreatic head posteriorly. However, to change the topographical anatomy of the superior and inferior arterial arcades into the final position, re-arrangement of the pancreatic parenchyma might be necessary in the head.
Keyword
MeSH Terms
Figure
-

Fig. 1 Horizontal sections showing early development of the arteries around the pancreatic head (9 weeks of gestation). (A) corresponds to the superiormost of the figure. Intervals between panels are 0.6 mm (A-B), 0.1 mm (B-C), 0.2 mm (C-D), 0.2 mm (D-E), 0.15 mm (E-F), 0.05 mm (F-G) and 0.1 mm (G-H), respectively. (A) displays the origin of the celiac trunk (CT). The left gastric artery (LGA) reached the stomach (S) in the same section because of the tortuous course. (B) 0.1 mm inferior to the origin of the superior mesenteric artery (SMA), the CT was already divided into the common hepatic artery (CHA) and splenic artery (SPA). (C) contains longitudinal sections of the right gastric artery (RGA) and common hepatic artery (CHA). Between panels B and C, the hepatoduodenal ligament reaches the liver hilar region. A thick bile duct in the liver hilar region (arrow in panel C) may be the primordium of the gall bladder. (D) exhibits the PSPDA and the gastroduodenal artery (GDA) in the anterior side of the pancreatic head (star). (E) suggests that the ventral and dorsal primordia of the pancreas were already fused. A wall of the portal vein (asterisk) was destroyed. (F, G and H) contains the right gastro-epiploic artery (RGEA) and ASPDA. (G) exhibits the minor duodenal papilla (minor p). In panels F and G, the splenic vein (SPV) is cut longitudinally and, in the immediately posterior side of the SMA, a tissue (asterisk) is lost in the histological procedure. The dorsal mesogastrium (black or white arrows in panel H) containing the pancreatic body (PB) is separated from the mesentery of the midgut containing the pancreatic head (star) by a narrow peritoneal space. All sections are of the same magnification (scale bar is shown in panel H). AG, adrenal gland (cortex); AO, aorta; BV, body of the vertebrae; CBD, common bile duct; CL, caudate lobe; D1 or D2, first or second portion of the duodenum; G, gonad and mesonephros; K, kidney; NC, prevertebral condensation of the neural crest-derived cells; PHA, proper hepatic artery; PY, pylorus; S3, segment III of the liver; SMV, superior mesenteric vein; SP, spleen; UV, umbilical vein.
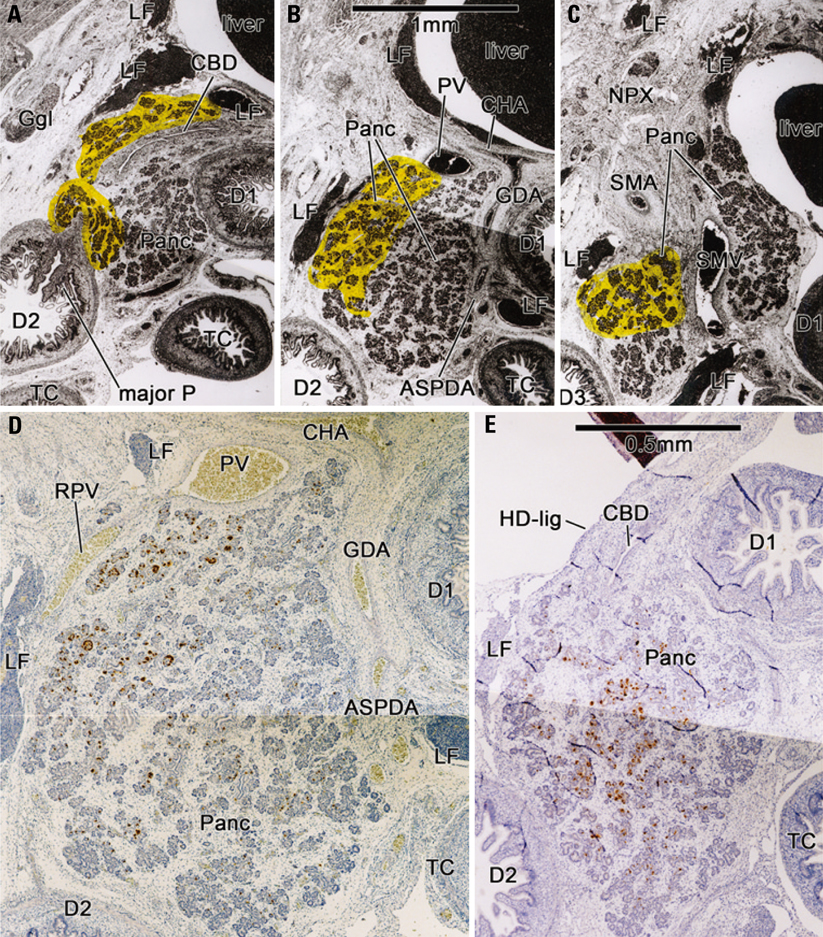
Fig. 2 Sagittal sections of the pancreatic head with pancreatic polypeptide (PP) immunohistochemistry (16 weeks of gestation). The left-hand side of the figures corresponds to the posterior side of the body. (A-E) displays the same fetus with 16 weeks of gestation. The PP immunoreactive areas are colored yellow in panels A-C, while the positive cells (brown-colored) are demonstrated in (D) and (E). (D), a near section of panel B, corresponds to the central part of (B). Interval between panels are 0.2 mm (A-B) and 0.6 mm (B-C), respectively (panel A is the right side of panels B and C). The PP immunoreactive areas are located along the common bile duct, in the posterosuperior part of the pancreatic head (Panc) and/or in the posterior side of the superior mesenteric vein (SMV). However, the area does not reach the inferior end of the head. The gastroduodenal artery and proximal course of the ASPDA do not attach to the PP immunoreactive cells (panels B, D and E). In (E) the negative immunoreactive parenchyma protruded inferiorly along the posterior aspect of the positive area. Note that the hepatoduodenal ligament (HD-lig) riding over the first portion of the duodenum (D1). D3, the third portion of the duodenum; Ggl, celiac ganglion; LF, lymph follicle; NPX, nerve plexus; PV, portal vein; RPV, retropancreatic vein; TC, transverse colon. Other abbreviations are the same as in Fig. 1. The magnification of panels A-C is different from (D) and (E) [scale bars, (B) and (E)].
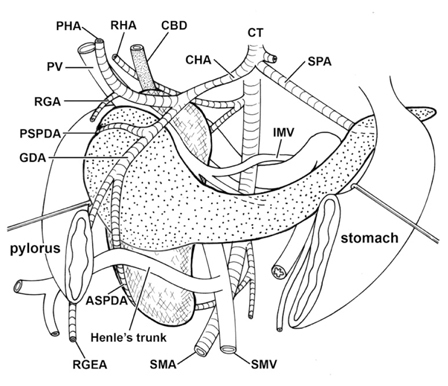
Fig. 3 A diagram showing arteries at and around the pancreatic head of a female fetus with 23 weeks of gestation. This diagram is based on observations of more than 200 horizontal sections of a fetus, parts of which will be shown in Fig. 5. The pancreas is composed of a transversely extending anterior mass (labeled by dots; almost corresponding to the dorsal pancreas) and a standing-up posterior mass of the pancreatic head (labeled by clusters of #; almost corresponding to the ventral pancreas). The hepatic artery (HA), portal vein (PV) and common bile duct (CBD) go superiorly and rightward across the superior side of the first portion of the duodenum. The right hepatic artery (RHA) originates from the superior mesenteric artery (SMA), issues the PIPDA and runs along the superior surface of the pancreatic head. The gastroduodenal artery (GDA) displayed a downward course. The PSPDA-PIPDA encircles the superior part of the pancreatic head, whereas the ASPDA-AIPDA runs around the inferiormost part. The inferior mesenteric vein (IMV) crosses the posterior aspect of the fourth portion of the duodenum. Because of a limitation of the drawing skill, the portal vein is separated from the pancreatic head in the inferior side of the figure. Other abbreviations are the same as in Fig. 1.
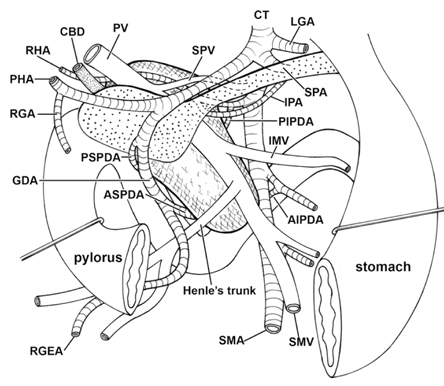
Fig. 4 A diagram showing arteries at and around the pancreatic head of a female fetus with 25 weeks of gestation. This diagram is based on observations of more than 200 horizontal sections of a fetus, parts of which will be shown in Fig. 6. In comparison with the diagram shown in Fig. 3, a transversely extending anterior mass of the pancreas (labeled by dots; almost corresponding to the dorsal pancreas) is slender while an obliquely positioned posterior mass [labeled by sharps (#); almost corresponding to the ventral pancreas] is thick. Arteries at and around the pancreatic head display courses similar to Fig. 3. The right hepatic artery (RHA) originates from the superior mesenteric artery (SMA) and issues the PIPDA and inferior pancreatic artery (IPA). The inferior mesenteric vein (IMV) crosses the anterior aspect of the fourth portion of the duodenum. Other abbreviations are the same as in Figs. 1 and 3.
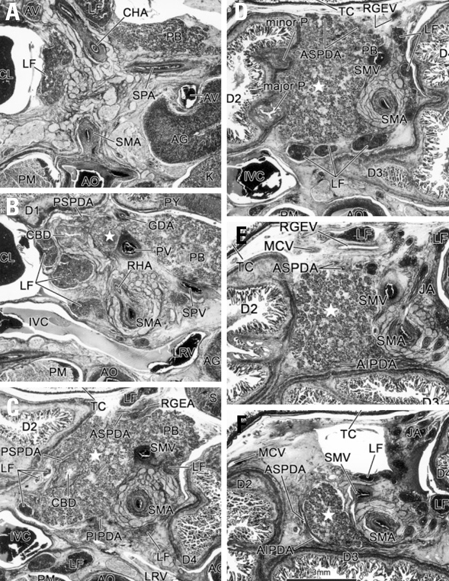
Fig. 5 Horizontal sections at and around the pancreatic head of a female fetus with the same 23 weeks-fetus as shown in Fig. 3. (A) corresponds to the superiormost of the figure. Intervals between panels are 2.2 mm (A-B), 1.8 mm (B-C), 2.0 mm (C-D), 1.1 mm (D-E), and 1.2 mm (E-F), respectively. (A) displays the splenic, common hepatic and superior mesenteric arteries near their origins (SPA, CHA, SMA). (B) exhibits the origin of the right hepatic artery (RHA) from the SMA. The gastroduodenal artery (GDA) and PSPDA are cut transversely in the anterior aspect of the pancreatic head (star). (C) shows origins of the right gastro-epiploic artery (RGEA) and ASPDA. The PSPDA is cut longitudinally and embedded in the superficial parenchyma of the pancreatic head (star). (D) displays the major and minor duodenal papillae (major p, minor p). Note that these two papillae are seen in a single horizontal section, not in a sagittal or frontal section. (E) contains the middle colic vein (MCV) and right gastroepiploic vein (RGEV) (i.e., Henle's gastrocolic venous trunk) and upper jejunal arteries (JA). (F) exhibits the ASPDA-AIPDA running around the inferiormost part of the pancreatic head (star). The SMA is surrounded by a thick nerve plexus (panels B-F). D1, D2, D3 and D4, the first-fourth portions of the duodenum; IVC, inferior vena cava; LF, lymph follicle; LRV, left renal vein; PM, psoas major; TC, transverse colon. Other abbreviations are the same as in Fig. 1.
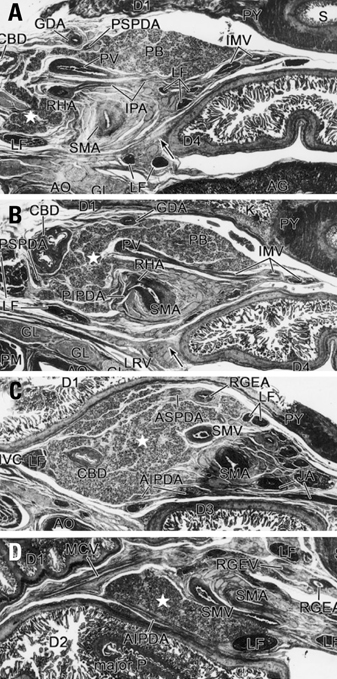
Fig. 6 Horizontal sections at and around the pancreatic head of a female fetus with the same 25 weeks-fetus as shown in Fig. 4. (A) corresponds to the superiormost of the figure. Intervals between panels are 0.9 mm (A-B), 2.0 mm (B-C) and 3.0 mm (C-D), respectively. (A) in the 6 mm inferior to the origin of the celiac trunk, displays the inferior pancreatic artery (IPA) arising from the right hepatic artery (RHA). (B) exhibits the origin of the RHA from the SMA. From the origin, the PIPDA is issued to the posterior side of the pancreatic head. In (B), the inferior mesenteric vein (IMV) is cut longitudinally and drains into the portal vein (PV). The fourth portion of the duodenum (D4) is connected by a tight connective tissue (arrow in panels A and B) to fasciae covering the left renal vein (LRV). (C) contains the ASPDA and right gastro-epiploic artery (RGEA). The upper jejunal artery (JA) issues the AIPDA. (D) displays the longitudinal sections of the ASPDA-AIPDA and Henle's venous trunk (the middle colic vein or MCV and the right gastro-epiploic vein or RGEV). Parts of the pancreatic head (star) are located in the posterior side of the superior mesenteric artery and vein because the vessels run transversely rather than inferiorly. LF, lymph follicle. Other abbreviations are the same as in Fig. 1.
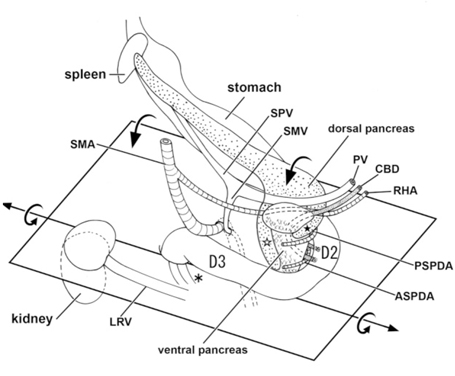
Fig. 7 A diagram showing joining processes between the dorsal and ventral primordia of the pancreas as well as the hypothetical rotation of the duodenum along a left-right axis. Viewed from the posterosuperior side of the body. A horizontal plane including most parts of the duodenum is shown to emphasize, in contrast to adults, the course of the second portion (D2) directing posteriorly rather than inferiorly. The topographical anatomy of the duodenum and pancreatic head is based on observations of fetuses of 20-30 weeks (e.g., Figs. 3, 4, 5 and 6). The anterior mass of the pancreatic head (labeled by dots) seems to correspond to the dorsal primordium of the pancreas, while an oblique or perpendicular posterior mass [labeled by sharps (#)] seems to primarily correspond to the ventral primordium. The portal vein and right hepatic artery run in the superior sides of and along their border between the anterior and posterior masses. Notably, tongue-like protrusions of the anterior mass or dorsal pancreas (stars) surround the primary posterior mass or the ventral pancreas. In particular, the right anterior protrusion (open star) often reaches the inferior end of the ventral pancreas. The common bile duct crosses the superior side of the first portion of the duodenum. We hypothesize a rotation along a left-right axis through the third portion of the duodenum in the later stage of development. In addition, the fourth portion is connected by a fascia (asterisk) to a thick fascia along the left renal vein.
Reference
-
1. Bertelli E, Di Gregorio F, Bertelli L, Mosca S. The arterial blood supply of the pancreas: a review. I. The superior pancreaticoduodenal and the anterior superior pancreaticoduodenal arteries. An anatomical and radiological study. Surg Radiol Anat. 1995. 17:97–106. 1–3.2. Bertelli E, Di Gregorio F, Bertelli L, Civeli L, Mosca S. The arterial blood supply of the pancreas: a review. II. The posterior superior pancreaticoduodenal artery. An anatomical and radiological study. Surg Radiol Anat. 1996. 18:1–9.3. Murakami G, Hirata K, Takamuro T, Mukaiya M, Hata F, Kitagawa S. Vascular anatomy of the pancreaticoduodenal region: a review. J Hepatobiliary Pancreat Surg. 1999. 6:55–68.
Article4. Sakamoto Y, Nagai M, Tanaka N, Nobori M, Tsukamoto T, Nokubi M, et al. Anatomical segmentectomy of the head of the pancreas along the embryological fusion plane: a feasible procedure? Surgery. 2000. 128:822–831.5. Paulin C, Dubois PM. Immunohistochemical identification and localization of pancreatic polypeptide cells in the pancreas and gastrointestinal tract of the human fetus and adult man. Cell Tissue Res. 1978. 188:251–257.
Article6. Rahier J, Wallon J, Gepts W, Haot J. Localization of pancreatic polypeptide cells in a limited lobe of the human neonate pancreas: remnant of the ventral primordium? Cell Tissue Res. 1979. 200:359–366.
Article7. Tadokoro H, Kozu T, Toki F, Kobayashi M, Hayashi N. Embryological fusion between the ducts of the ventral and dorsal primordia of the pancreas occurs in two manners. Pancreas. 1997. 14:407–414.
Article8. Uchida T, Takada T, Ammori BJ, Suda K, Takahashi T. Three-dimensional reconstruction of the ventral and dorsal pancreas: a new insight into anatomy and embryonic development. J Hepatobiliary Pancreat Surg. 1999. 6:176–180.9. Takada T. Vantral pancreatectomy: resection of the ventral segment of the pancreas. J Hepatobiliary Pancreat Surg. 1993. 1:36–40.10. Ryu M, Takayama W, Watanabe K, Honda I, Yamamoto H, Arai Y. Ventral pancreatic resection for adenoma and low-grade malignancies of the head of the pancreas. Surg Today. 1996. 26:476–481.11. Takahashi S, Akita K, Goseki N, Sato T. Spatial arrangement of the pancreatic ducts in the head of the pancreas with special reference to the branches of the uncinate process. Surgery. 1999. 125:178–185.12. Kamisawa T, Egawa N, Tu Y, Tsuruta K, Okamoto A. Pancreatographic investigation of embryology of complete and incomplete pancreas divisum. Pancreas. 2007. 34:96–102.13. Michels NA. Blood supply and anatomy of the upper abdominal organs with a descriptive atlas. 1955. Philadelphia: Lippincott;24–133.14. Adda G, Hannoun L, Loygue J. Development of the human pancreas: variations and pathology. A tentative classification. Anat Clin. 1984. 5:275–283.15. Krakowiak-Sarnowska E, Flisiñski P, Szpinda M, Flisiński M, Sarnowski J. The pancreaticodudenal arteries in human foetal development. Folia Morphol (Warsz). 2004. 63:281–284.16. Skandalakis JE, Gray SW. Embryology for surgeons: the embryological basis for the treatment of congenital anomalies. 1994. Baltimore: Williams & Wilkins;396–404.17. Lee SD, Kim CY, Cho YH, Fujiwara D, Murakami G, Mutsumura H, et al. Morphometrical data of size and shape of the late-stage human fetal liver, including those of intrahepatic vessels: some prenatal and postnatal developmental consideration. Korean J Hepatobiliary Pancreat Surg. 2003. 7:12–18.18. Kanagasuntheram R. Some observations on the development of the human duodenum. J Anat. 1960. 94:231–240.19. Kimura W, Nagai H. Study of surgical anatomy for duodenum-preserving resection of the head of the pancreas. Ann Surg. 1995. 221:359–363.
Article20. Furukawa H, Iwata R, Moriyama N, Kosuge T. Blood supply to the pancreatic head, bile duct, and duodenum: evaluation by computed tomography during arteriography. Arch Surg. 1999. 134:1086–1090.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vascular Anatomy of the Pancreaticoduodenal Region
- Duodenum-preserving Pancreatic Head Resection for Benign Pancreatic Head Lesion
- Pancreatic Head Resection with Segmental Duodenectomy
- Experiences with Pancreaticoduodenal Injuries at a Single Institute
- Topographical Morphology of the Lingual Artery in Korean
