Artificial External Glottic Device for Passive Lung Insufflation
- Affiliations
-
- 1Department of Rehabilitation Medicine, College of Medicine, Kyung Hee University, Seoul, Korea.
- 2Department of Rehabilitation Medicine and Rehabilitation Institute of Muscular Disease, Yonsei University College of Medicine, Seoul, Korea. skyler02@wku.ac.kr
- 3Department of Family Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1058818
- DOI: http://doi.org/10.3349/ymj.2011.52.6.972
Abstract
- PURPOSE
For patients with neuromuscular disease, air stacking, which inflates the lungs to deep volumes, is important for many reasons. However, neuromuscular patients with severe glottic dysfunction or indwelling tracheostomy tubes cannot air stack effectively. For these patients, we developed a device that permits deep lung insufflations substituting for glottic function.
MATERIALS AND METHODS
Thirty-seven patients with bulbar-innervated muscle weakness and/or tracheostomies were recruited. Twenty-three had amyotrophic lateral sclerosis, and 14 were tetraplegic patients due to cervical spinal cord injury. An artificial external glottic device (AEGD) was used to permit passive deep lung insufflation. In order to confirm the utility of AEGD, vital capacity, maximum insufflation capacity (MIC), and lung insufflation capacity (LIC) with AEGD (LICA) were measured.
RESULTS
For 30 patients, MICs were initially zero. However, with the use of the AEGD, LICA was measurable for all patients. The mean LICA was 1,622.7+/-526.8 mL. Although MIC was measurable for the remaining 7 patients without utilizing the AEGD, it was significantly less than LICA, which was 1,084.3+/-259.9 mL and 1,862.9+/-248 mL, respectively (p<0.05).
CONCLUSION
The AEGD permits lung insufflation by providing deeper lung volumes than possible by air stacking.
MeSH Terms
Figure
-

Fig. 1 A fully assembled apparatus for measuring LIC with the artificial external glottic device (LICA): a resuscitation bag is connected to the AEGD. Connection part (A); Control part (B). LIC, lung insufflation capacity; AEGD, artificial external glottic device; LICA, LIC with AGED.
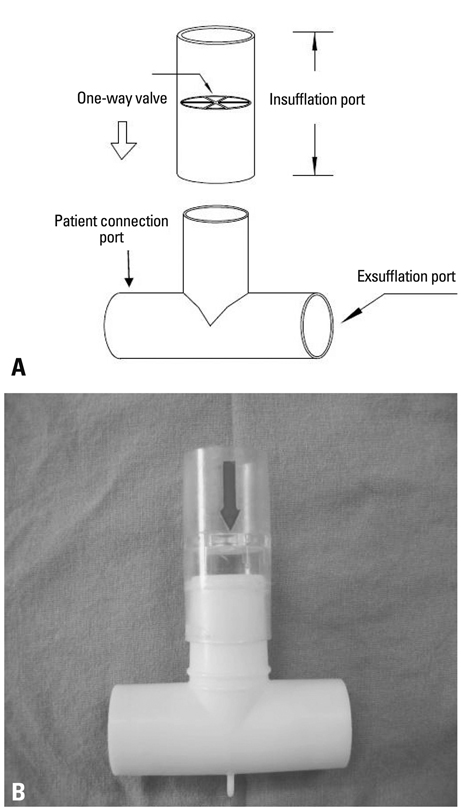
Fig. 2 Connection part of the artificial external glottic device (AEGD). (A) Disconnected view of the connection part. (B) Photograph of the connection part.
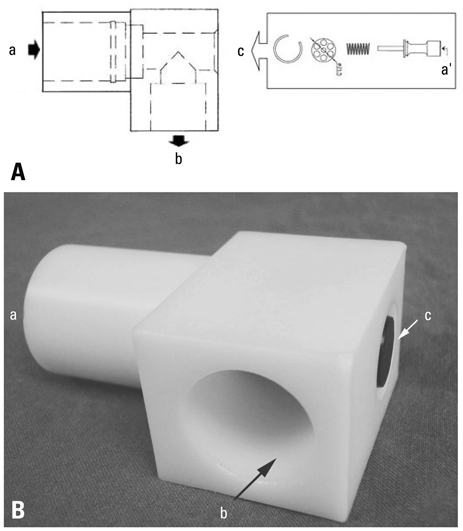
Fig. 3 Diagram of the control part of the artificial external glottic device (AEGD). (A) Demounted view of the control part: control part is connected to the connection part through (a), and measurement apparatus such as a spirometer through (b), the external glottic function is controlled by an externally exposed part (c) of the pushing bar a', air flows from (a) to (b) like an opening of a normal glottis. (B) Photograph of the control part of AEGD: ports connecting to the connection part (a); to the measurement apparatus such as a spirometer (b); and to the external control of the glottis (c).
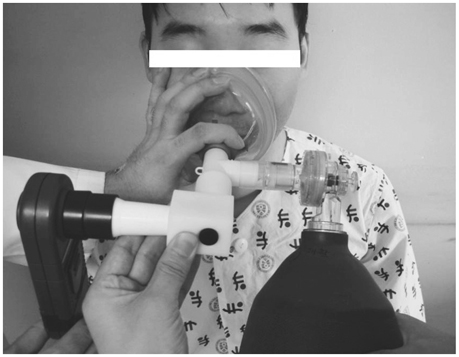
Fig. 4 Actual application of the apparatus for the measurement of LICA. LICA, LIC with AEGD.
Reference
-
1. Kang SW, Bach JR. Maximum insufflation capacity. Chest. 2000. 118:61–65.
Article2. Estenne M, Heilporn A, Delhez L, Yernault JC, De Troyer A. Chest wall stiffness in patients with chronic respiratory muscle weakness. Am Rev Respir Dis. 1983. 128:1002–1007.3. Estenne M, Gevenois PA, Kinnear W, Soudon P, Heilporn A, De Troyer A. Lung volume restriction in patients with chronic respiratory muscle weakness: the role of microatelectasis. Thorax. 1993. 48:698–701.
Article4. Hoffman LA. Ineffective airway clearance related to neuromuscular dysfunction. Nurs Clin North Am. 1987. 22:151–166.5. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in neuromuscular disease. Am J Phys Med Rehabil. 2000. 79:222–227.6. Bach JR, Bianchi C, Vidigal-Lopes M, Turi S, Felisari G. Lung inflation by glossopharyngeal breathing and "air stacking" in Duchenne muscular dystrophy. Am J Phys Med Rehabil. 2007. 86:295–300.
Article7. Bach JR, Mahajan K, Lipa B, Saporito L, Goncalves M, Komaroff E. Lung insufflation capacity in neuromuscular disease. Am J Phys Med Rehabil. 2008. 87:720–725.
Article8. Leith DE. Brain JD, Proctor D, Reid L, editors. Cough. Lung biology in health and disease. 1977. New York: Marcel Dekker;545–592.9. Similowski T, Attali V, Bensimon G, Salachas F, Mehiri S, Arnulf I, et al. Diaphragmatic dysfunction and dyspnoea in amyotrophic lateral sclerosis. Eur Respir J. 2000. 15:332–337.
Article10. Hanayama K, Ishikawa Y, Bach JR. Amyotrophic lateral sclerosis. Successful treatment of mucous plugging by mechanical insufflation-exsufflation. Am J Phys Med Rehabil. 1997. 76:338–339.11. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory flows with manually assisted and unassisted coughing techniques. Chest. 1993. 104:1553–1562.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Device for Improving Cough Function: Through Assisting Glottic Function
- Fatal Venous Air Embolism during Lung Surgery
- Use of a trans-tracheal rapid insufflation of oxygen device in a “cannot intubate, cannot oxygenate†scenario in a parturient: a case report
- Differences of Hemodynamics and Arterial Blood Gas in Right and Left Lung Ventilation during Thoracoscopic Surgery with CO2 Insufflation
- Hemodynamic and Arterial Blood Gas Changes during Thoracoscopic Surgery with CO2 Insufflation Under GEneral Anesthesia
