A Case of Crystalline Keratopathy in Monoclonal Gammopathy of Undetermined Significance (MGUS)
- Affiliations
-
- 1Department of Ophthalmology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. jck50ey@kornet.net
- KMID: 1010029
- DOI: http://doi.org/10.3341/kjo.2011.25.3.202
Abstract
- A 62-year-old female visited our clinic with progressively decreased vision in both eyes beginning 12 years prior. Idiopathic corneal opacity in all layers of the cornea was found in both eyes. One year later, we performed penetrating keratoplasty on the undiagnosed right eye. During post-surgical follow-up, corneal edema and stromal opacity recurred, and penetrating keratoplasty was performed two more times. The patient's total serum protein level, which had previously been normal, was elevated prior to the final surgery. She was diagnosed with monoclonal gammopathy of undetermined significance. We made a final diagnosis of monoclonal gammopathy-associated crystalline keratopathy after corneal biopsy. Monoclonal gammopathy-associated crystalline keratopathy is difficult to diagnose and may lead to severe visual loss. A systemic work-up, including serologic tests like serum protein or cholesterol levels, is needed in patients with unexplainable corneal opacity.
Keyword
MeSH Terms
-
Corneal Edema/etiology/*metabolism/physiopathology/surgery
Corneal Neovascularization/etiology/*metabolism/physiopathology/surgery
Corneal Opacity/etiology/*metabolism/physiopathology/surgery
Crystallins/*metabolism
Female
Humans
Keratoplasty, Penetrating
Microscopy, Electron
Middle Aged
Monoclonal Gammopathy of Undetermined Significance/*complications/pathology
Reoperation
Visual Acuity
Figure
-
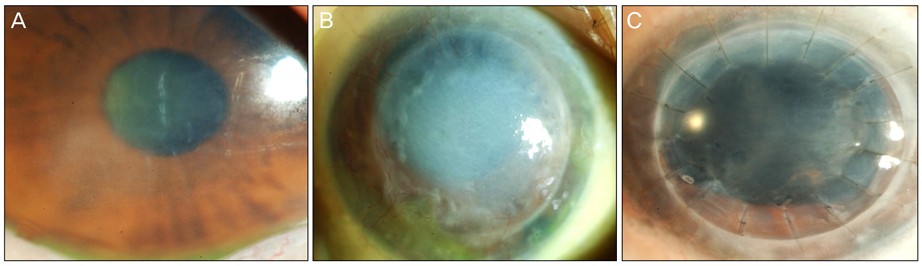
Fig. 1 Slit-lamp photographs of recurring corneal opacity in a crystalline keratopathy patient with monoclonal gammopathy of undetermined significance despite keratoplasty surgeries. (A) Before the penetrating keratoplasty, corneal stromal edema, opacity and Descemet's folds presented in both eyes. (B) Four years after the first surgery, corneal opacity recurred in the right eye. (C) Photograph showing corneal opacity two years after the second keratoplasty.
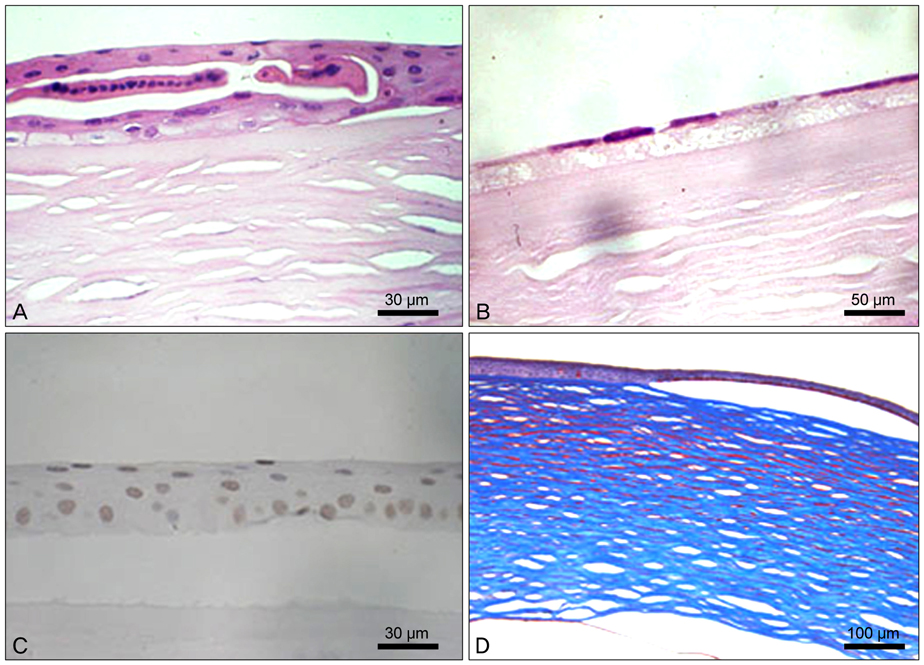
Fig. 2 Corneal biopsy photographs from a crystalline keratopathy patient. (A) Hematoxylin and eosin staining showing loss of polarity, with clusters in the epithelium (×100). (B) Hematoxylin and eosin staining showing a decreased number of endothelial cells with some vacuoles in Descemet's membrane (×40). (C) TUNEL staining showing increased keratocyte apoptosis with condensed nuclei (×100). (D) Masson trichrome staining showing deposits in the corneal stroma (×40).
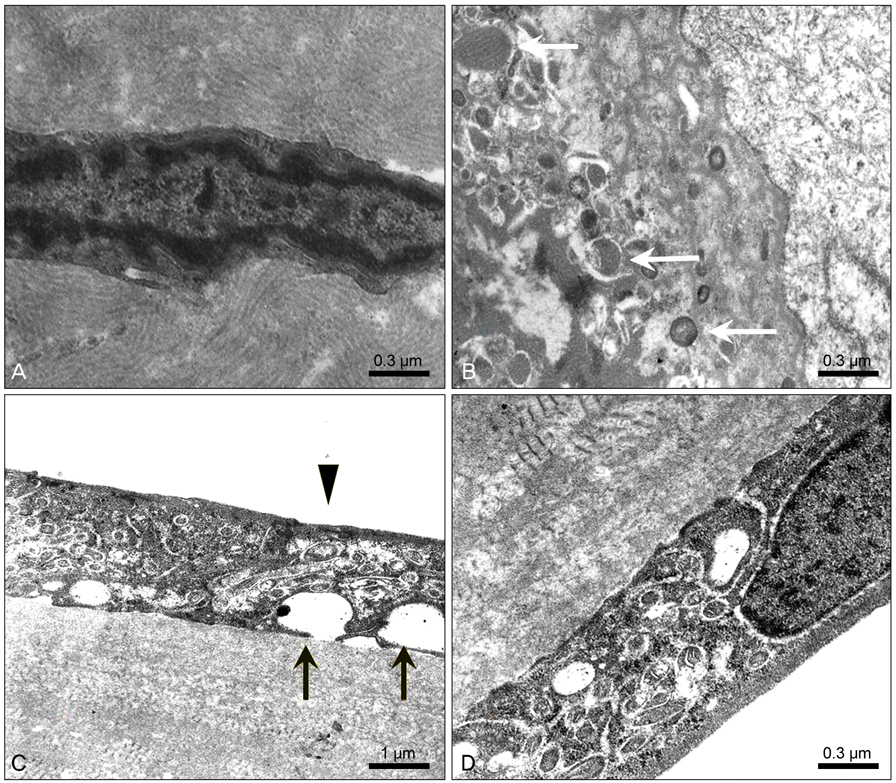
Fig. 3 Electron microscopic photographs of crystalline keratopathy. (A) Microtubular crystal deposits were found around a keratocyte whose chromatin was condensed (×28,000). (B) Crystal deposits phagocytosed by a macrophage (white arrow) (×28,000). (C) Vacuoles in the endothelium (black arrow) and loss of microvilli (arrow head) (×10,000). (D) Abnormal banded collagen fibrils were seen with a background of amorphous material in the posterior portion of Descemet's membrane (×28,000).
Reference
-
1. Kyle RA. 'Benign' monoclonal gammopathy. A misnomer? JAMA. 1984. 251:1849–1854.2. Kyle RA, Rajkumar SV. Monoclonal gammopathy of undetermined significance and smoldering multiple myeloma. Hematol Oncol Clin North Am. 2007. 21:1093–1113. ix3. Garibaldi DC, Gottsch J, de la Cruz Z, et al. Immunotactoid keratopathy: a clinicopathologic case report and a review of reports of corneal involvement in systemic paraproteinemias. Surv Ophthalmol. 2005. 50:61–80.4. Klintworth GK, Bredehoeft SJ, Reed JW. Analysis of corneal crystalline deposits in multiple myeloma. Am J Ophthalmol. 1978. 86:303–313.5. Choi HW, Lee SJ, Park JM, Kim WS. A case of multiple myeloma presented with bilateral corneal crystalline deposition. J Korean Ophthalmol Soc. 2009. 50:1266–1269.6. Barr CC, Gelender H, Font RL. Corneal crystalline deposits associated with dysproteinemia. Report of two cases and review of the literature. Arch Ophthalmol. 1980. 98:884–889.7. Graichen DF, Perez E, Jones DB, Font RL. kappa-Immunoglobulin corneal deposits associated with monoclonal gammopathy. Immunohistochemical and electron microscopic findings. Ger J Ophthalmol. 1994. 3:54–57.8. Ormerod LD, Collin HB, Dohlman CH, et al. Paraproteinemic crystalline keratopathy. Ophthalmology. 1988. 95:202–212.9. Spiegel P, Grossniklaus HE, Reinhart WJ, Thomas RH. Unusual presentation of paraproteinemic corneal infiltrates. Cornea. 1990. 9:81–85.10. Sekundo W, Seifert P. Monoclonal corneal gammopathy: topographic considerations. Ger J Ophthalmol. 1996. 5:262–267.11. Moller HU, Ehlers N, Bojsen-Moller M, Ridgway AE. Differential diagnosis between granular corneal dystrophy Groenouw type I and paraproteinemic crystalline keratopathy. Acta Ophthalmol (Copenh). 1993. 71:552–555.12. Barr CC, Gelender H, Font RL. Corneal crystalline deposits associated with dysproteinemia. Report of two cases and review of the literature. Arch Ophthalmol. 1980. 98:884–889.13. Kyle RA. "Benign" monoclonal gammopathy: after 20 to 35 years of follow-up. Mayo Clin Proc. 1993. 68:26–36.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chronic Demyelinating Neuropathy associated with IgG lamda Type Monoclonal Gammopathy of Undetermined Significance
- Dysphagia as a Clinical Manifestation of Monoclonal Gammopathy of Undetermined Significance: A Case Report
- Generalized Plane Xanthoma Associated with Monoclonal Gammopathy of Unknown Significance
- A Case of Diffuse Plane Xanthoma Associated with Monoclonal Gammopathy of Unknown Significance and Normolipoproteinemia
- Monoclonal Gammopathy of Undetermined Significance Presented as a Vasculitic Neuropathy
