J Korean Orthop Assoc.
2007 Apr;42(2):264-269. 10.4055/jkoa.2007.42.2.264.
Causes and Surgical Treatment of Idiopathic Genu Vara
- Affiliations
-
- 1Department of Orthopedic Surgery, Yonsei University College of Medicine, Seoul, Korea. pedhkim@yumc.yonsei.ac.kr
- 2Department of Orthopedic Surgery, Hallym University College of Medicine, Anyang, Korea.
- KMID: 854597
- DOI: http://doi.org/10.4055/jkoa.2007.42.2.264
Abstract
- PURPOSE: To determine the underlying causes of idiopathic genu vara, and to evaluate the results of surgery. MATERIALS AND METHODS: Radiographic measurements were made using a standing orthoroentgenogram and a computerized axial tomography scan. Functional and cosmetic results after surgery were evaluated according to the causes. RESULTS: The patients with idiopathic genu vara were categorized into three groups: a group associated with increased femoral anteversion, a group associated with tibia vara and increased external rotation of the tibia, and a group associated with tibia vara. Satisfactory functional and cosmetic results were obtained after corrective surgery based on actual causes. CONCLUSION: An accurate analysis based on the rotational and angular deformities is needed to make a surgical treatment plan for idiopathic genu vara.
Keyword
Figure
-
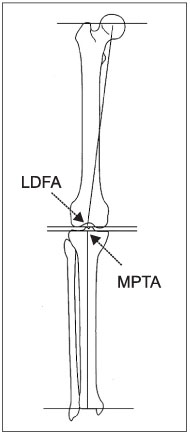
Fig. 1 Frontal plane joint orientation angle relative to the mechanical axis. LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle.
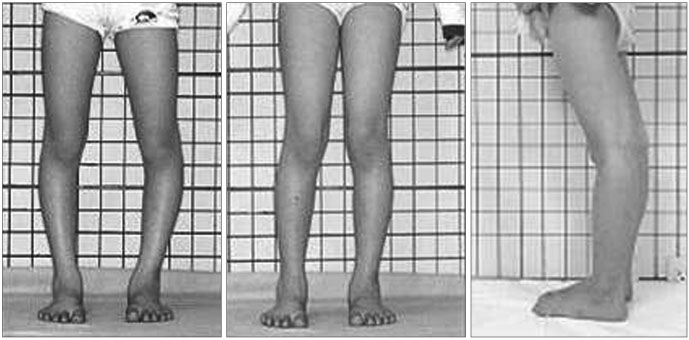
Fig. 2 A 9 year-old boy in Group I. Inwardly pointing patellar due to increased femoral anteversion, which was assumed to be an apparent genu vara. A normal alignment of the lower extremity was observed when patellar was pointed forward. Genu recurvatum was also frequent in this group.
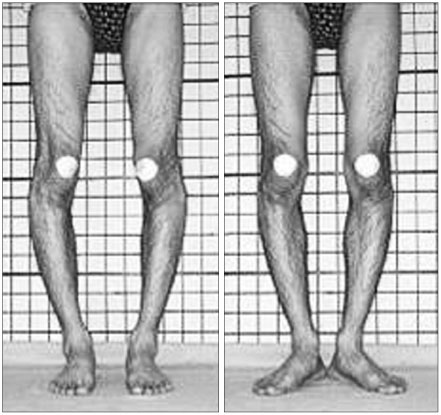
Fig. 3 A 18 year-old student in Group II. Tibia vara and increased external rotation of the tibia were obseved when the patellar was pointed forward.
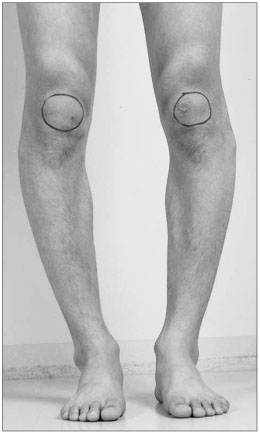
Fig. 4 A 21 year-old student in Group III. Only tibia vara was observed when the patellar was pointed forward.
Reference
-
1. Alvik I. Increased anteversion of the femur as the only manifestation of dysplasia of the hip. Clin Orthop Relat Res. 1962. 22:16–20.2. Cooke TD, Price N, Fisher B, Hedden D. The inwardly pointing knee. An unrecognized problem of external rotational malalignment. Clin Orthop Relat Res. 1990. 260:56–60.3. Delgado ED, Schoenecker PL, Rich MM, Capelli AM. Treatment of severe torsional malalignment syndrome. J Pediatr Orthop. 1996. 16:484–488.
Article4. Eckhoff DG, Kramer RC, Alongi CA, VanGerven DP. Femoral anteversion and arthritis of the knee. J Pediatr Orthop. 1994. 14:608–610.
Article5. Fabry G, MacEwen GD, Shands AR Jr. Torsion of the femur. A follow-up study in normal and abnormal conditions. J Bone Joint Surg Am. 1973. 55:1726–1738.6. Halpern AA, Tanner J, Rinsky L. Does persistent fetal femoral anteversion contribute to osteoarthritis?: a preliminary report. Clin Orthop Relat Res. 1979. 145:213–216.7. Herzenberg JE, Smith JD, Paley D. Correcting torsional deformities with Ilizarov's apparatus. Clin Orthop Relat Res. 1994. 302:36–41.8. Heller MO, Bergmann G, Deuretzbacher G, Claes L, Haas NP, Duda GN. Influence of femoral anteversion on proximal femoral loading: measurement and simulation in four patients. Clin Biomech [Bristol, Avon]. 2001. 16:644–649.
Article9. James SL. Kennedy JC, editor. Chondromalacia of the patella in the adolescent. The injured adolescent knee. 1979. Baltimore: Williams & Wilkins;205–251.10. Kitaoka HB, Weiner DS, Cook AJ, Hoyt WA, Askew MJ. Relationship between femoral anteversion and osteoarthritis of the hip. J Pediatr Orthop. 1989. 9:396–404.
Article11. Kling TF Jr, Hensinger RN. Angular and torsional deformities of the lower limbs in children. Clin Orthop Relat Res. 1983. 176:136–147.
Article12. Krengel WF 3rd, Staheli LT. Tibial rotational osteotomy for idiopathic torsion. A comparison of the proximal and distal osteotomy levels. Clin Orthop Relat Res. 1992. 283:285–289.13. Lee TQ, Anzel SH, Bennett KA, Pang D, Kim WC. The influence of fixed rotational deformities of the femur on the patellofemoral contact pressures in human cadaver knees. Clin Orthop Relat Res. 1994. 302:69–74.
Article14. Meister K, James SL. Proximal tibial derotation osteotomy for anterior knee pain in the miserably malaligned extremity. Am J Orthop. 1995. 24:149–155.15. Paley D, Herzenberg JE, Testworth K, McKie J, Bhave A. Deformity planing for frontal and sagittal plane corrective osteotomies. Orthop Clin North Am. 1994. 25:425–465.16. Shtarker H, Volpin G, Stolero J, Kaushansky A, Samchukov M. Correction of combined angular and rotational deformities by the Ilizarov method. Clin Orthop Relat Res. 2002. 402:184–195.
Article17. Staheli LT. Rotational problems in children. Instr Course Lect. 1994. 43:199–209.
Article18. Svenningsen S, Apalset K, Terjesen T, Anda S. Osteotomy for femoral anteversion. Complications in 95 children. Acta Orthop Scand. 1989. 60:401–405.
Article19. Turner MS, Smillie IS. The effect of tibial torsion of the pathology of the knee. J Bone Joint Surg Br. 1981. 63:396–398.
Article20. Visser JD, Jonkers A, Hillen B. Hip joint measurements with computerized tomography. J Pediatr Orthop. 1982. 2:143–146.
Article21. Wedge JH, Munkacsi I, Loback D. Anteversion of the femur and idiopathic osteoarthrosis of the hip. J Bone Joint Surg Am. 1989. 71:1040–1043.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A New Classification for Idiopathic Genu Vara
- A Child with Familial Hypophosphatemic Ricket: A case report
- Surgical Treatment of Habitual Patella Dislocation with Genu Valgum
- The Efficacy of Percutaneous Lateral Hemiepiphysiodesis on Angular Correction in Idiopathic Adolescent Genu Varum
- Combined Abduction and Derotation Osteotomy in Bilateral Congenital Coxa Bara Vara: Report of Bilateral Treatment
