Efficacy of PEEK Cages and Plate Augmentation in Three-Level Anterior Cervical Fusion of Elderly Patients
- Affiliations
-
- 1Depatment of Orthopaedic Surgery, Chonbuk National University Hospital & Research Institute of Clinical Medicine, Chonbuk National University School of Medicine, Jeonju, Korea. docby@hanmail.net
- KMID: 999455
- DOI: http://doi.org/10.4055/cios.2011.3.1.9
Abstract
- BACKGROUND
To evaluate the clinical efficacy of three-level anterior cervical arthrodesis with polyethyletherketone (PEEK) cages and plate fixation for aged and osteoporotic patients with degenerative cervical spinal disorders.
METHODS
Twenty one patients, who had undergone three-level anterior cervical arthrodesis with a cage and plate construct for degenerative cervical spinal disorder from November 2001 to April 2007 and were followed up for at least two years, were enrolled in this study. The mean age was 71.7 years and the mean T-score using the bone mineral density was -2.8 SD. The fusion rate, change in cervical lordosis, adjacent segment degeneration were analyzed by plain radiographs and computed tomography, and the complications were assessed by the medical records. The clinical outcomes were analyzed using the SF-36 physical composite score (PCS) and neck disability index (NDI).
RESULTS
Radiological fusion was observed at a mean of 12.3 weeks (range, 10 to 15 weeks) after surgery. The average angle of cervical lordosis was 5degrees preoperatively, 17.6degrees postoperatively and 16.5degrees at the last follow-up. Degenerative changes in the adjacent segments occurred in 3 patients (14.3%), but revision surgery was unnecessary. In terms of instrument-related complications, there was cage subsidence in 5 patients (23.8%) with an average of 2.8 mm, and loosening of the plate and screw occurred in 3 patients (14.3%) but there were no clinical problems. The SF-36 PCS before surgery, second postoperative week and at the last follow-up was 29.5, 43.1, and 66.2, respectively. The respective NDI was 55.3, 24.6, and 15.9.
CONCLUSIONS
For aged and osteoporotic patients with degenerative cervical spinal disorders, three-level anterior cervical arthrodesis with PEEK cages and plate fixation reduced the pseudarthrosis and adjacent segment degeneration and improved the clinical outcomes. This method is considered to be a relatively safe and effective treatment modality.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Biocompatible Materials
*Bone Plates/adverse effects
Bone Screws/adverse effects
Cervical Vertebrae/radiography/*surgery
Diskectomy
Female
Follow-Up Studies
Humans
Ketones
Lordosis/pathology
Male
Radiculopathy/surgery
Severity of Illness Index
Spinal Cord Diseases/surgery
Spinal Diseases/*surgery
Spinal Fusion/adverse effects/*methods
Treatment Outcome
Figure
-
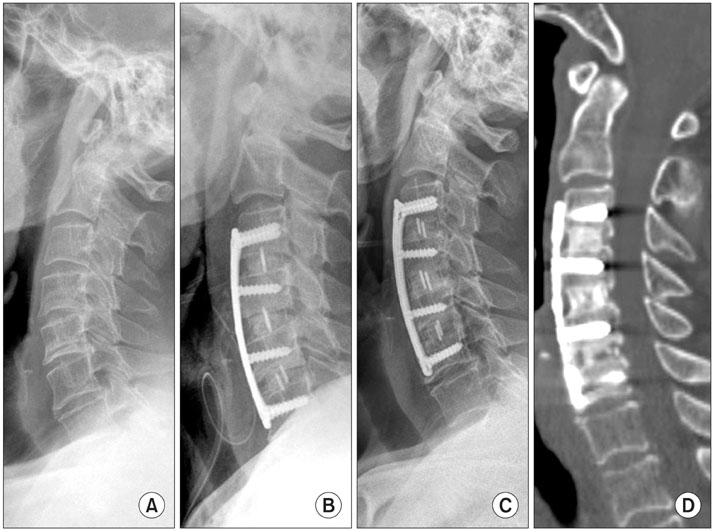
Fig. 1 A sixty-nine-year-old woman who had pain in the neck and radiculopathy. (A) Lateral roentgenogram showing narrowing of the disc space and posterior osteophytes from the third to the sixth cervical vertebrae. (B) Lateral roentgenogram taken one day after anterior cervical arthrodesis with a cage and plate construct at C3-4, C4-5, and C5-6. (C) Four years later, lateral roentgenogram showing a solid fusion and physiologic lordosis. (D) Four years later, computed tomogram showing a solid fusion at the C3-4, C4-5, and C5-6 fusion levels.

Fig. 2 A seventy-four-year-old woman who had suffered from cervical myelopathy. (A) Lateral roentgenogram showing local kyphosis and narrowing of the disc space from the fourth to the seventh cervical vertebrae. (B) Lateral roentgenogram taken one day after an anterior cervical arthrodesis with a cage and plate construct at C4-5, C5-6, and C6-7. (C) Three years later, lateral roentgenogram showing a cage subsidence at C6-7 fusion level, but showing a solid union. (D) Three years later, computed tomogram showing cage subsidence and fibrous union at the C6-7 fusion level.
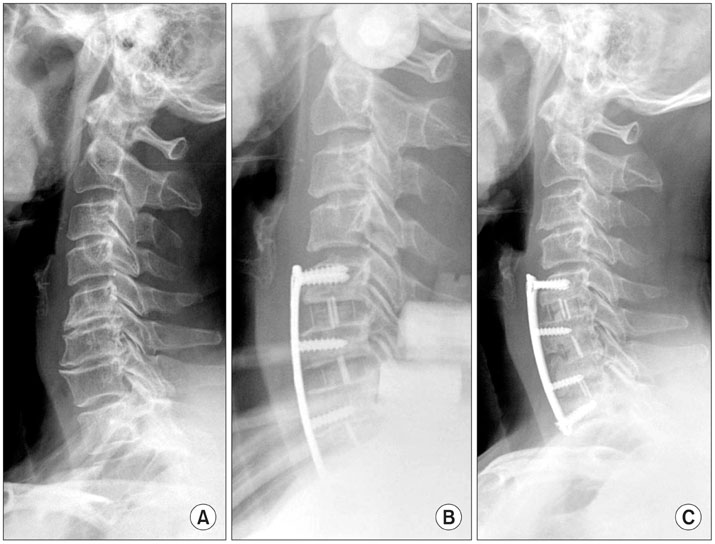
Fig. 3 A sixty-six-year-old woman who had pain in the neck and radiculopathy. (A) Lateral roentgenogram showing narrowing of the disc space and posterior osteophytes from the fifth cervical vertebra to the first thoracic vertebra. (B) Lateral roentgenogram taken one day after anterior cervical arthrodesis with a cage and plate construct at the C5-6, C6-7, and C7-T1 levels. (C) Thirty-two months later, lateral roentgenogram showing loosening of a plate and screw at C5 but no neurologic complications occurred.
Reference
-
1. Celik SE, Kara A, Celik S. A comparison of changes over time in cervical foraminal height after tricortical iliac graft or polyetheretherketone cage placement following anterior discectomy. J Neurosurg Spine. 2007. 6(1):10–16.
Article2. Demircan MN, Kutlay AM, Colak A, et al. Multilevel cervical fusion without plates, screws or autogenous iliac crest bone graft. J Clin Neurosci. 2007. 14(8):723–728.
Article3. Xie Y, Chopin D, Hardouin P, Lu J. Clinical, radiological and histological study of the failure of cervical interbody fusions with bone substitutes. Eur Spine J. 2006. 15(8):1196–1203.
Article4. Liao JC, Niu CC, Chen WJ, Chen LH. Polyetheretherketone (PEEK) cage filled with cancellous allograft in anterior cervical discectomy and fusion. Int Orthop. 2008. 32(5):643–648.
Article5. Cho DY, Lee WY, Sheu PC. Treatment of multilevel cervical fusion with cages. Surg Neurol. 2004. 62(5):378–385.
Article6. Cho DY, Liau WR, Lee WY, Liu JT, Chiu CL, Sheu PC. Preliminary experience using a polyetheretherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery. 2002. 51(6):1343–1349.
Article7. Gercek E, Arlet V, Delisle J, Marchesi D. Subsidence of stand-alone cervical cages in anterior interbody fusion: warning. Eur Spine J. 2003. 12(5):513–516.
Article8. Kulkarni AG, Hee HT, Wong HK. Solis cage (PEEK) for anterior cervical fusion: preliminary radiological results with emphasis on fusion and subsidence. Spine J. 2007. 7(2):205–209.
Article9. Lee SH, Suk KS, Kim KT, Lee JH, Seo EM, Im YS. Outcome analysis of single level anterior cervical fusion using interbody PEEK cage with autologous iliac bone graft. J Korean Orthop Assoc. 2009. 44(1):93–101.
Article10. Mastronardi L, Ducati A, Ferrante L. Anterior cervical fusion with polyetheretherketone (PEEK) cages in the treatment of degenerative disc disease: preliminary observations in 36 consecutive cases with a minimum 12-month follow-up. Acta Neurochir (Wien). 2006. 148(3):307–312.
Article11. Meier U, Kemmesies D. Experiences with six different intervertebral disc spacers for spondylodesis of the cervical spine. Orthopade. 2004. 33(11):1290–1299.12. Kim KT, Suk KS, Kim JM. Future development of interbody fusion cages. J Korean Soc Spine Surg. 2001. 8(3):386–391.
Article13. Song KJ, Lee KB. A preliminary study of the use of cage and plating for single-segment fusion in degenerative cervical spine disease. J Clin Neurosci. 2006. 13(2):181–187.
Article14. Emery SE, Fisher JR, Bohlman HH. Three-level anterior cervical discectomy and fusion: radiographic and clinical results. Spine (Phila Pa 1976). 1997. 22(22):2622–2624.15. Barsa P, Suchomel P. Factors affecting sagittal malalignment due to cage subsidence in standalone cage assisted anterior cervical fusion. Eur Spine J. 2007. 16(9):1395–1400.
Article16. Schmieder K, Wolzik-Grossmann M, Pechlivanis I, Engelhardt M, Scholz M, Harders A. Subsidence of the wing titanium cage after anterior cervical interbody fusion: 2-year follow-up study. J Neurosurg Spine. 2006. 4(6):447–453.
Article17. Robinson RA, Smith GW. Anterolateral cervical disk removal and interbody fusion for cervical disk syndrome. Bull Johns Hopkins Hosp. 1955. 96(5):223–224.18. Kandziora F, Pflugmacher R, Scholz M, et al. Treatment of traumatic cervical spine instability with interbody fusion cages: a prospective controlled study with a 2-year follow-up. Injury. 2005. 36:Suppl 2. B27–B35.
Article19. Koller H, Hempfing A, Ferraris L, Maier O, Hitzl W, Metz-Stavenhagen P. 4- and 5-level anterior fusions of the cervical spine: review of literature and clinical results. Eur Spine J. 2007. 16(12):2055–2071.
Article20. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 1999. 81(4):519–528.
Article21. Farey ID, McAfee PC, Davis RF, Long DM. Pseudarthrosis of the cervical spine after anterior arthrodesis. Treatment by posterior nerve-root decompression, stabilization, and arthrodesis. J Bone Joint Surg Am. 1990. 72(8):1171–1177.
Article22. Bohlman HH, Emery SE, Goodfellow DB, Jones PK. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy. Long-term follow-up of one hundred and twenty-two patients. J Bone Joint Surg Am. 1993. 75(9):1298–1307.
Article23. Bohler J, Gaudernak T. Anterior plate stabilization for fracture-dislocation of the lower cervical spine. J Trauma. 1980. 20(3):203–205.24. Emery SE, Bolesta MJ, Banks MA, Jones PK. Robinson anterior cervical fusion comparison of the standard and modified techniques. Spine (Phila Pa 1976). 1994. 19(6):660–663.25. Papadopoulos EC, Huang RC, Girardi FP, Synnott K, Cammisa FP Jr. Three-level anterior cervical discectomy and fusion with plate fixation: radiographic and clinical results. Spine (Phila Pa 1976). 2006. 31(8):897–902.26. Wang JC, McDonough PW, Kanim LE, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for three-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 2001. 26(6):643–646.
Article27. Hwang SL, Lee KS, Su YF, et al. Anterior corpectomy with iliac bone fusion or discectomy with interbody titanium cage fusion for multilevel cervical degenerated disc disease. J Spinal Disord Tech. 2007. 20(8):565–570.
Article28. Natarajan RN, Chen BH, An HS, Andersson GB. Anterior cervical fusion: a finite element model study on motion segment stability including the effect of osteoporosis. Spine (Phila Pa 1976). 2000. 25(8):955–961.29. van Jonbergen HP, Spruit M, Anderson PG, Pavlov PW. Anterior cervical interbody fusion with a titanium box cage: early radiological assessment of fusion and subsidence. Spine J. 2005. 5(6):645–649.
Article30. Malloy KM, Hilibrand AS. Autograft versus allograft in degenerative cervical disease. Clin Orthop Relat Res. 2002. (394):27–38.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Efficacy of Cages in Anterior Cervical Fusion for Degenerative Cervical Disease
- Stand-Alone Cervical Cages in 2-Level Anterior Interbody Fusion in Cervical Spondylotic Myelopathy: Results from a Minimum 2-Year Follow-up
- Comparison between Two Different Cervical Interbody Fusion Cages in One Level Stand-alone ACDF: Carbon Fiber Composite Frame Cage Versus Polyetheretherketone Cage
- Two-Level Anterior Cervical Discectomy and Fusion with Stand-alone Cages in Cervical Spinal Degenerative Diseases
- The Comparison of Multi-level Fusion versus One-level Fusion to the Development of Adjacent Level Degeneration in Anterior Cervical Arthrodesis with PEEK Cage and Plate Augmentation for the Degenerative Cervical Spinal Disorders
