The Volume of Tumor Mass and Visual Field Defect in Patients with Pituitary Macroadenoma
- Affiliations
-
- 1Department of Ophthalmology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea. eyechung90@hallym.or.kr
- KMID: 994410
- DOI: http://doi.org/10.3341/kjo.2011.25.1.37
Abstract
- PURPOSE
We used the Swedish interactive threshold algorithms (SITA) standard strategy of Humphrey perimetry, to analyze the pattern of visual field (VF) defects and evaluate the quantitative correlation between the tumor volume and severity of VF defects in patients with pituitary macroadenoma.
METHODS
We reviewed 50 patients with pituitary macroadenoma who received VF test and 11 patients were excluded. VF analysis was performed with Humphrey perimeter using the SITA standard strategy. The tumor volume was assessed radiologically via brain magnetic resonance images and was calculated using Cavalieri's principle. We used the mean deviation (MD) and pattern standard deviation (PSD) of the Humphrey parameter to measure VF defect severity, and then analyzed the correlation of tumor volume with VF defects.
RESULTS
Twenty nine patients (74%) showed abnormal VF and bitemporal field changes, which were the most common field defects on presentation. Seven patients (18%) had unilateral VF defects, 22 patients (56%) had bilateral VF defects. The tumor volume of the patients with VF defects was significantly larger than that of patients with normal VF (p = 0.006). The tumor volume exhibited significant negative correlation with MD (r = -0.693; p < 0.001) and significant positive correlation with PSD (r = 0.589; p < 0.001).
CONCLUSIONS
In patients with pituitary macroadenoma, there was a variety of VF defects and a high correlation between the tumor volume and the severity of VF defects. SITA standard strategy can be a fast and quantitative method for evaluating central VF defects.
Keyword
MeSH Terms
Figure
-
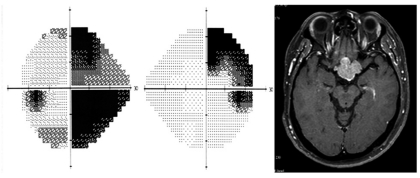
Fig. 1 Humphrey visual field shows right incongruous homonymous hemianopia. Gadolinium-enhanced, T1-weighted magnetic resonance images of the brain reveal a mass that involves the optic tract.
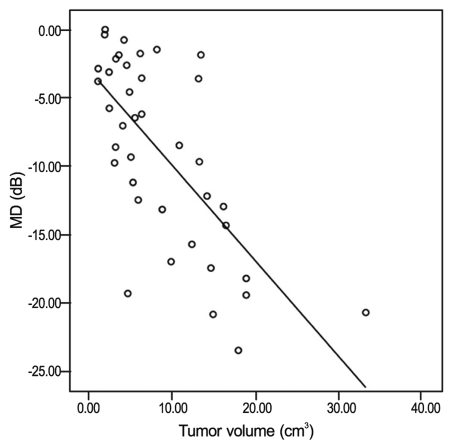
Fig. 2 Correlation between mean deviation (MD) and tumor volume in patients with pituitary macroadenoma. Pearson correlation coefficient = -0.693, p < 0.001.

Fig. 3 Correlation between pattern standard deviation (PSD) and tumor volume in patients with pituitary macroadenoma. Pearson correlation coefficient = 0.589, p < 0.001.
Cited by 1 articles
-
The Influence of Pituitary Adenoma Size on Vision and Visual Outcomes after Trans-Sphenoidal Adenectomy: A Report of 78 Cases
Ren-Wen Ho, Hsiu-Mei Huang, Jih-Tsun Ho
J Korean Neurosurg Soc. 2015;57(1):23-31. doi: 10.3340/jkns.2015.57.1.23.
Reference
-
1. Anderson D, Faber P, Marcovitz S, et al. Pituitary tumors and the ophthalmologist. Ophthalmology. 1983; 90:1265–1270. PMID: 6664664.
Article2. Hennessey JV, Jackson IM. Clinical features and differential diagnosis of pituitary tumours with emphasis on acromegaly. Baillieres Clin Endocrinol Metab. 1995; 9:271–314. PMID: 7625986.
Article3. Hollenhorst RW, Younge BR. Kohler PO, Ross GT, editors. Ocular manifestations produced by adenomas of the pituitary gland: analysis of 1000 cases. Diagnosis and treatment of pituitary tumors. 1973. Amsterdam: Excerpta Medica;p. 53–59.4. Ebersold MJ, Quast LM, Laws ER Jr, et al. Long-term results in transsphenoidal removal of nonfunctioning pituitary adenomas. J Neurosurg. 1986; 64:713–719. PMID: 3701419.
Article5. Poon A, McNeill P, Harper A, O'Day J. Patterns of visual loss associated with pituitary macroadenomas. Aust N Z J Ophthalmol. 1995; 23:107–115. PMID: 7546685.
Article6. Rivoal O, Brézin AP, Feldman-Billard S, Luton JP. Goldmann perimetry in acromegaly: a survey of 307 cases from 1951 through 1996. Ophthalmology. 2000; 107:991–997. PMID: 10811095.7. Donahue SP. Perimetry techniques in neuro-ophthalmology. Curr Opin Ophthalmol. 1999; 10:420–428. PMID: 10662247.
Article8. Mills RP. Automated perimetry in neuro-ophthalmology. Int Ophthalmol Clin. 1991; 31:51–70. PMID: 1743895.
Article9. Fujimoto N, Saeki N, Miyauchi O, Adachi-Usami E. Criteria for early detection of temporal hemianopia in asymptomatic pituitary tumor. Eye (Lond). 2002; 16:731–738. PMID: 12439668.
Article10. Beck RW, Bergstrom TJ, Lichter PR. A clinical comparison of visual field testing with a new automated perimeter, the Humphrey Field Analyzer, and the Goldmann perimeter. Ophthalmology. 1985; 92:77–82. PMID: 3974997.
Article11. Wong AM, Sharpe JA. A comparison of tangent screen, goldmann, and humphrey perimetry in the detection and localization of occipital lesions. Ophthalmology. 2000; 107:527–544. PMID: 10711892.12. Bengtsson B, Olsson J, Heijl A, Rootzén H. A new generation of algorithms for computerized threshold perimetry, SITA. Acta Ophthalmol Scand. 1997; 75:368–375. PMID: 9374242.
Article13. Thomas R, Shenoy K, Seshadri MS, et al. Visual field defects in non-functioning pituitary adenomas. Indian J Ophthalmol. 2002; 50:127–130. PMID: 12194569.14. Levy MJ, Jäger HR, Powell M, et al. Pituitary volume and headache: size is not everything. Arch Neurol. 2004; 61:721–725. PMID: 15148150.15. Miller NR, Walsh FB, Hoyt WF. Walsh and Hoyt's clinical neuro-ophthalmology. 2005. 6th ed. Baltimore: Lipponcott Williams & Wilkins;p. 503–573.16. Hershenfeld SA, Sharpe JA. Monocular temporal hemianopia. Br J Ophthalmol. 1993; 77:424–427. PMID: 8343470.
Article17. Nishimura M, Kurimoto T, Yamagata Y, et al. Giant pituitary adenoma manifesting as homonymous hemianopia. Jpn J Ophthalmol. 2007; 51:151–153. PMID: 17401630.
Article18. Katz J, Tielsch JM, Quigley HA, Sommer A. Automated perimetry detects visual field loss before manual Goldmann perimetry. Ophthalmology. 1995; 102:21–26. PMID: 7831036.
Article19. Trope GE, Britton R. A comparison of Goldmann and Humphrey automated perimetry in patients with glaucoma. Br J Ophthalmol. 1987; 71:489–493. PMID: 3307897.
Article20. Szatmáry G, Biousse V, Newman NJ. Can Swedish interactive thresholding algorithm fast perimetry be used as an alternative to goldmann perimetry in neuro-ophthalmic practice? Arch Ophthalmol. 2002; 120:1162–1173. PMID: 12215089.
Article21. Gedik S, Gur S, Atalay B, et al. Humphrey visual field analysis, visual field defects, and ophthalmic findings in patients with macro pituitary adenoma. Saudi Med J. 2007; 28:1380–1384. PMID: 17768464.22. Stewart WC, Hunt HH. Threshold variation in automated perimetry. Surv Ophthalmol. 1993; 37:353–361. PMID: 8484168.
Article23. Heijl A, Drance SM. Changes in differential threshold in patients with glaucoma during prolonged perimetry. Br J Ophthalmol. 1983; 67:512–516. PMID: 6871143.
Article24. Bengtsson B, Heijl A, Olsson J. Evaluation of a new threshold visual field strategy, SITA, in normal subjects. Swedish interactive thresholding algorithm. Acta Ophthalmol Scand. 1998; 76:165–169. PMID: 9591946.25. Sekhar GC, Naduvilath TJ, Lakkai M, et al. Sensitivity of Swedish interactive threshold algorithm compared with standard full threshold algorithm in Humphrey visual field testing. Ophthalmology. 2000; 107:1303–1308. PMID: 10889102.
Article26. Budenz DL. Atlas of visual fields. 1997. Philadelphia: Lippincott-Raven;p. 1–77.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intrasellar Cavernous Hemangioma
- The Efficacy of Radiation Therapy in the Treatment of Pituitary Adenoma
- Pituitary Apoplexy due to Pituitary Adenoma Infarction
- The Influence of Pituitary Adenoma Size on Vision and Visual Outcomes after Trans-Sphenoidal Adenectomy: A Report of 78 Cases
- Pituicytoma with Significant Tumor Vascularity Mimicking Pituitary Macroadenoma
